Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 55(2); 2022 > Article
-
Original Article
Spatio-temporal Distribution of Suicide Risk in Iran: A Bayesian Hierarchical Analysis of Repeated Cross-sectional Data -
Seyed Saeed Hashemi Nazari1
 , Kamyar Mansori2, Hajar Nazari Kangavari3, Ahmad Shojaei4, Shahram Arsang-Jang2,5
, Kamyar Mansori2, Hajar Nazari Kangavari3, Ahmad Shojaei4, Shahram Arsang-Jang2,5 -
Journal of Preventive Medicine and Public Health 2022;55(2):164-172.
DOI: https://doi.org/10.3961/jpmph.21.385
Published online: February 10, 2022
1Safety Promotion and Injury Prevention Research Center, Department of Epidemiology, School of Public Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Epidemiology and Biostatistics, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran
3Department of Epidemiology, School of Public Health, Iran University of Medical Sciences, Tehran, Iran
4Legal Medicine Research Center, Iranian Legal Medicine Organization, Tehran, Iran
5Department of Epidemiology and Biostatistics, Faculty of Medicine, Qom University of Medical Sciences, Qom, Iran
- Corresponding author: Shahram Arsang-Jang, Department of Epidemiology and Biostatistics, Faculty of Medicine, Qom University of Medical Sciences, Shahid Lavasani Street, Qom 37100, Iran, E-mail: shahramarsang@gmail.com
Copyright © 2022 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- We aimed to estimate the space-time distribution of the risk of suicide mortality in Iran from 2006 to 2016.
-
Methods
- In this repeated cross-sectional study, the age-standardized risk of suicide mortality from 2006 to 2016 was determined. To estimate the cumulative and temporal risk, the Besag, York, and Mollié and Bernardinelli models were used.
-
Results
- The relative risk of suicide mortality was greater than 1 in 43.0% of Iran’s provinces (posterior probability >0.8; range, 0.46 to 3.93). The spatio-temporal model indicated a high risk of suicide in 36.7% of Iran’s provinces. In addition, significant upward temporal trends in suicide risk were observed in the provinces of Tehran, Fars, Kermanshah, and Gilan. A significantly decreasing pattern of risk was observed for men (β, −0.013; 95% credible interval [CrI], −0.010 to −0.007), and a stable pattern of risk was observed for women (β, −0.001; 95% CrI, −0.010 to 0.007). A decreasing pattern of suicide risk was observed for those aged 15–29 years (β, −0.006; 95% CrI, −0.010 to −0.0001) and 30–49 years (β, −0.001; 95% CrI, −0.018 to −0.002). The risk was stable for those aged >50 years.
-
Conclusions
- The highest risk of suicide mortality was observed in Iran’s northwestern provinces and among Kurdish women. Although a low risk of suicide mortality was observed in the provinces of Tehran, Fars, and Gilan, the risk in these provinces is increasing rapidly compared to other regions.
- Suicide mortality is a major public health issue, and approximately 800 000 suicide deaths are recorded every year. The global suicide rate was estimated to be 10.6 deaths per 100 000 population in 2016, with 77% of suicides occurring in low-income and middle-income countries [1]. Different patterns of suicide have been observed in various parts of the world [2].
- In addition to psychological factors and socio-demographic characteristics [3], spatial [4] and temporal differences [5,6] also play an important role in the occurrence of suicidal phenomena. Suicide rates do not only differ by country [7]. Evidence has also suggested that the suicide rate varies across geographic regions and based on the spatial environment within a country, such as urban and rural areas and different states or provinces [8]. In addition, some evidence indicates a positive relationship between suicide and changes in the regional climate [9].
- The results of a study conducted by the Forensic Medicine Research Center found that the suicide rate in Iran was around 5 deaths per 100 000 population nationwide, and although the rate was lower than the majority of other countries worldwide, especially Western nations, it is still considered high relative to other Middle Eastern countries [1]. The particular conditions related to the suicide rate at the province level within a country vary, and some provinces face critical conditions that lead to increases in the rate of suicide. Moreover, trends in the suicide rates of different provinces have fluctuated over the past 10 years [10]. A study of data from Ilam Province used spatial-temporal analysis to examine the incidence of suicide attempts in its cities to identify regional differences in suicide rates [11].
- Therefore, it is important to study the suicide rate in Iran from a spatial and temporal perspective. Identifying the provinces with upward trends in the suicide rate will enable studies investigating causality in these areas in the future. In addition, the study results will significantly help to determine spatio-temporal discrepancies in the suicide rate of Iran and improve our understanding of the success of large-scale health policies to address this issue and direct attention to the provinces with the most need. Analysis of the existing data by credible organizations regionally and overall can effectively increase our knowledge of the epidemiology of suicide and effective health planning to reduce the burden of suicide on the health systems in Iran’s provinces. In addition, such an analysis can provide valuable information about the possible geographic patterns of suicide death in Iran.
- Given the significance and sensitivity of suicide-related phenomena, as well as temporal and spatial changes in suicide rates, the present study was developed with the objective of analyzing the epidemiology of suicide deaths, comparing the incidence rate by age and gender across all of Iran’s provinces from 2006 to 2016. We aimed to map the suicide mortality rate locally and temporally and identify high-risk regions using Bayesian statistical methods.
INTRODUCTION
- This repeated cross-sectional study was conducted from 2006 to 2016 using data on suicide mortality from the Legal Medicine Organization of Iran. Suicide mortality data were extracted according to the International Statistical Classification of Diseases and Related Health Problems classification system. The national database was compiled based on mandatory notifications from regional Legal Medicine Organization of Iran facilities across all 31 provinces, with annual data being aggregated from each district. All confirmed instances of suicide mortality among individuals of both genders aged 15 years or older were included. Suicide mortality was examined using a nationally representative sample at the regional level as well by area of residence (urban or rural).
- We used the Iran Statistical Center database to extract information about population size, including the total population and the population in each province by gender and year.
- The World Health Organization (WHO) standard population was used to estimate the population for each age group. The number of suicide deaths was used as the outcome variable. Confirmed suicide deaths among those aged 15 years or older of both genders were included. The age-standardized mortality rate based on the WHO standard population was used to identify risk of suicide mortality hotspots.
- We estimated relative risk (RR) to measure the risk of suicide mortality. In the hierarchical model for estimating the RR, we included the random intercept and logarithm of the expected number of suicide deaths in each province as an offset.
- If yit indicates the recorded number of suicide deaths in it province during year t, then, considering the population at risk (Rit) and rate of suicide at year t (rt), the corresponding age-/gender-specific expected suicide mortality rate (Eit) is given by;
- The standardized ratio of yit to Eit is the maximum likelihood estimator for the area-specific RR. To estimate the cumulative risk, the Besag, York, and Mollié (BYM) model was used to examine 11-year aggregate data. To model the suicide risk according to the prior distribution of suicide deaths in neighboring regions as well as temporal factors, the Bernardinelli model (1995) was used. The observed number of suicide deaths was modeled using conditionally-independent Poisson random variables in a generalized linear model using the log link function.
- To estimate the RR (θi) by province (i), a combination of spatial components (intrinsic conditional auto-regressive [CAR] ϑi) and random effects components for non-spatial heterogeneity (ui) was used in the BYM model:
- The overall nationwide RR indicated the suicide mortality rate across the country, with the exponential of intercept (α). For each region, the RR showed either an increase or decrease in suicide mortality compared to the nationwide suicide mortality rate. If the 95% credible interval (CrI) of the RR did not include 1, there was considered to be strong statistical evidence for the significance of the RR.
- In the Bernardinelli model, we examined the hypothesis that there would be a stable trend in suicide mortality over time using the temporal trend (TT), which included both the overall time trend and the area-specific time trend. A positive value for the slope of a province’s trend was considered to indicate a more rapid increase in suicide mortality compared to the overall trend.
- The logarithm to determine the RR was as follows:
- with α indicating the intercept, ui and ϑi indicating the random effects of areas, β indicating the overall linear trend effect, and δi indicating the possible interaction between area and time. The observed and expected number of suicides in each region were included in the Poisson model in addition to the correlated and non-correlated inhomogeneity indices for each region. δi, ϑi, and ui were included in the model to measure the temporal effect, correlated inhomogeneity, and non-correlated inhomogeneity in each region, respectively. We considered a CAR distribution for non-correlated inhomogeneity. In addition, the effect for each region had a normal distribution with harmonic means on the neighboring regions.
- To analyze the space-time interaction for detecting possible temporal patterns, posterior probability (PP) was used, with values closer to 1 indicating a more unstable temporal pattern [12].
- We defined the prior gamma distribution for the total variance of the model. We used the reverse distribution of gamma (0.0005) and alpha (0.5) with a normally distributed mean and CAR-normal distribution considering a prior distribution with a mean of 0. Bayesian post probability was also used to calculate the p-values, which were used to compare the RRs with 1 as well as to determine the significance of the RR. The Markov-chain Monte Carlo method was applied for data fitting. The RR, TT, and differential trend (DT) were estimated based on the model. To determine the performance of the model, Golman-Roubin diagrams were used while the deviance information criterion was used for comparing the models and selecting the final model. Sensitivity analyses was performed to compare the consistency of main model estimates with the results of the restricted model. Also to select the optimal hyper-priors and hyper-parameters for the model.
- OpenBUGS was used to conduct the statistical analyses, and the results were plotted in ArcGIS.
- Ethics Statement
- The study protocol was reviewed and approved by the Qom University of Medical Sciences (No. IR.MUQ.REC.1396.39). In addition, the aggregate data was used with no individual identifiers.
METHODS
- Overall Suicide Rate
- According to the results of the BYM model, which was based on aggregate data, the RR of suicide was greater than 1 in approximately 43% of Iran’s provinces (PP>0.8), with their RRs varying from 0.46 to 3.93.
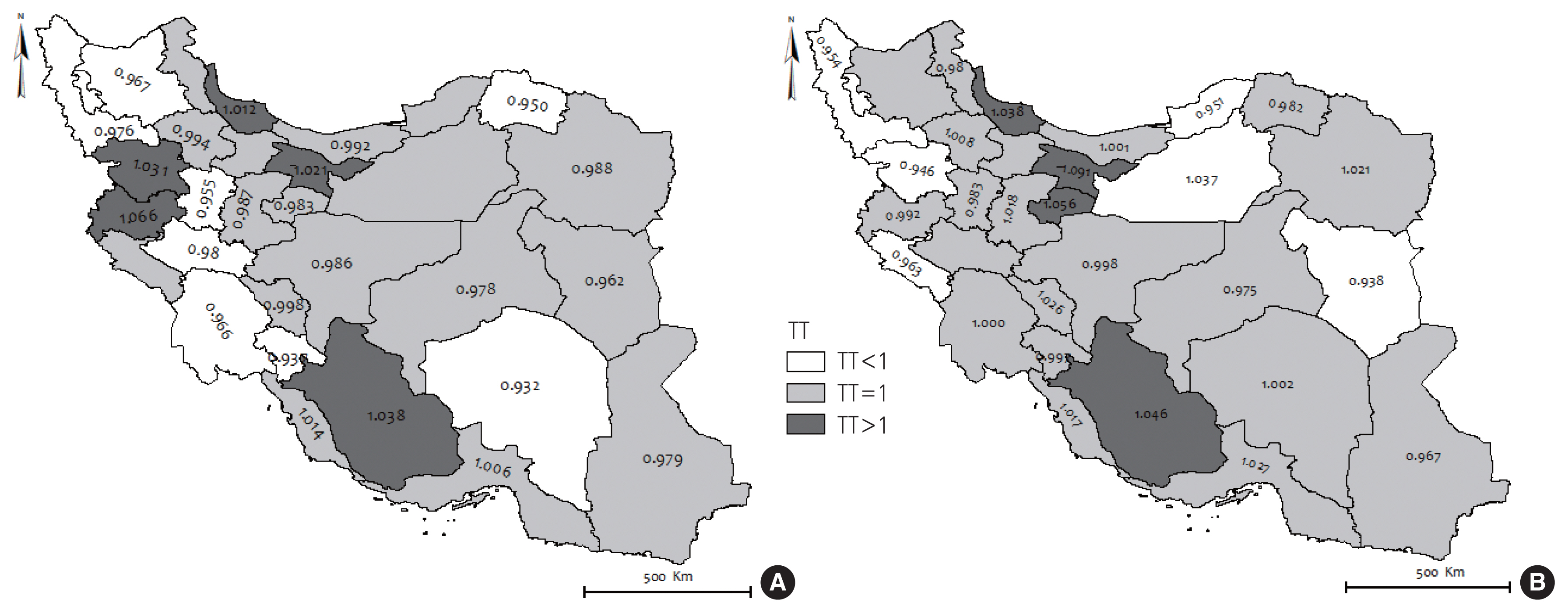
- The results of the spatio-temporal model indicated that the suicide risk was significantly greater than 1 in 11 provinces (36.7%) (Figure 1A). In addition, significantly upward TTs in the suicide risk were observed in the provinces of Tehran (P28), Fars (P7), Kermanshah (P15), and Gilan (P9). The trend of the suicide risk was stable in 15 (50.0%) provinces (Figure 1B).
- The DT results were similar to the results of the analysis of TTs. The estimated DT and corresponding Bayesian PP values suggested that the trends in the suicide risk in the provinces of Tehran (P28), Fars (P7), Kermanshah (P15), and Gilan (P9) were significantly steeper than the nationwide trend (Supplemental Material 1).
- Suicide Risk by Gender
- Not accounting for TTs, the cumulative incidence rate of suicide in Iran was 6.75 deaths per 100 000 population for men 2.88 deaths per 100 000 population for women from 2006 to 2016. According to the results of the BYM model, the cumulative RRs were significantly greater than 1 in 10 provinces (33.3%) for women, and the RR was highest in Ilam (P13; RR, 5.92) followed by Kermanshah (P15; RR, 4.26), Lorestan (P22; RR, 3.65) and Kohkiluyeh-Buyerahmad (P20; RR, 2.03). The cumulative RRs were significantly greater than 1 in 11 provinces (36.4%) for mens, and the RR was highest in Kermanshah (P15; RR, 3.25) followed by Ilam (P13; RR, 2.98), Hamadan (P11; RR, 2.17), and Lorestan (P22; RR, 2.00) over the 10-year study period (Supplemental Material 1).
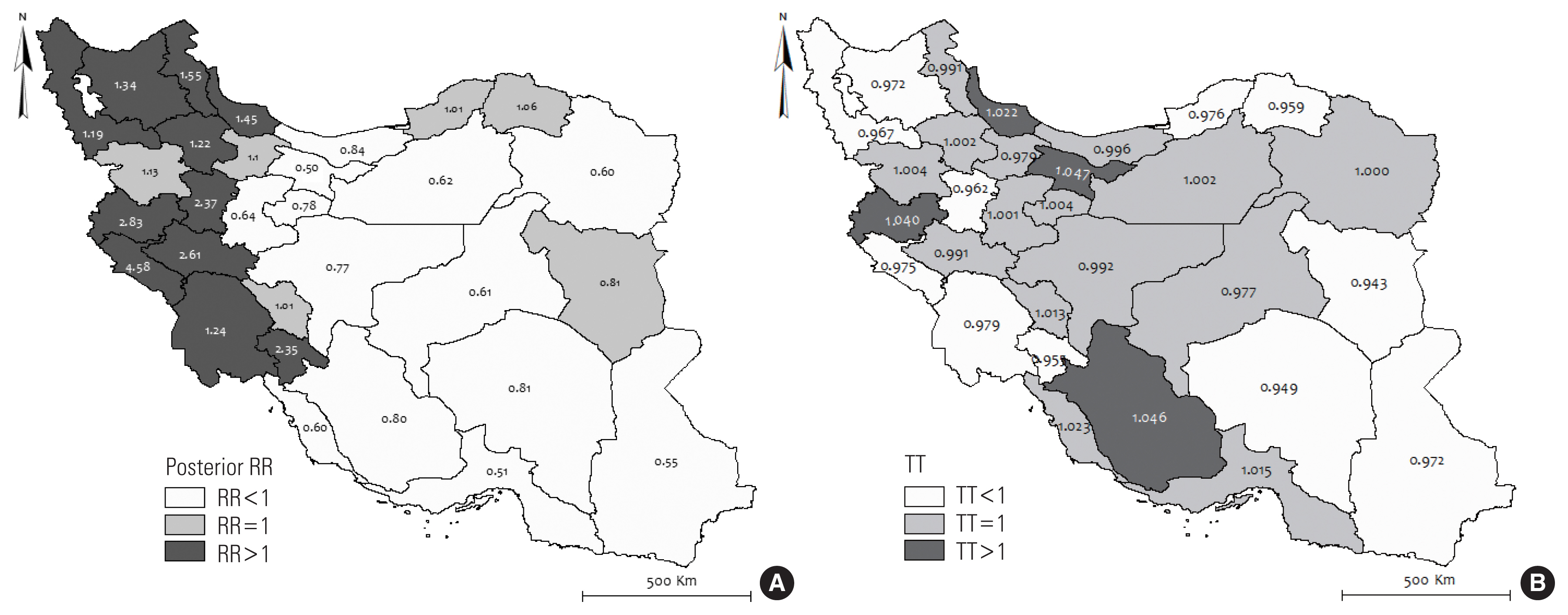
- Figure 2 shows the RRs derived from the spatio-temporal model according to gender and province. Although the results show a significantly decreasing pattern of risk among men (β, 0.013; 95% CrI, −0.010 to −0.007), a stable pattern of risk was observed among women (β, −0.001; 95% CrI, −0.010 to 0.007).
- For men, the trend of the suicide risk in the provinces of Kermanshah (P15), Fars (P7), Kurdistan (P21), Tehran (P28), and Gilan (P9) was significantly steeper than the nationwide trend. For women, the trend of the suicide risk in the provinces of Tehran (P28), Fars (P7), Gilan (P9), and Qom (25) was significantly steeper than the nationwide trend (Supplemental Material 1).
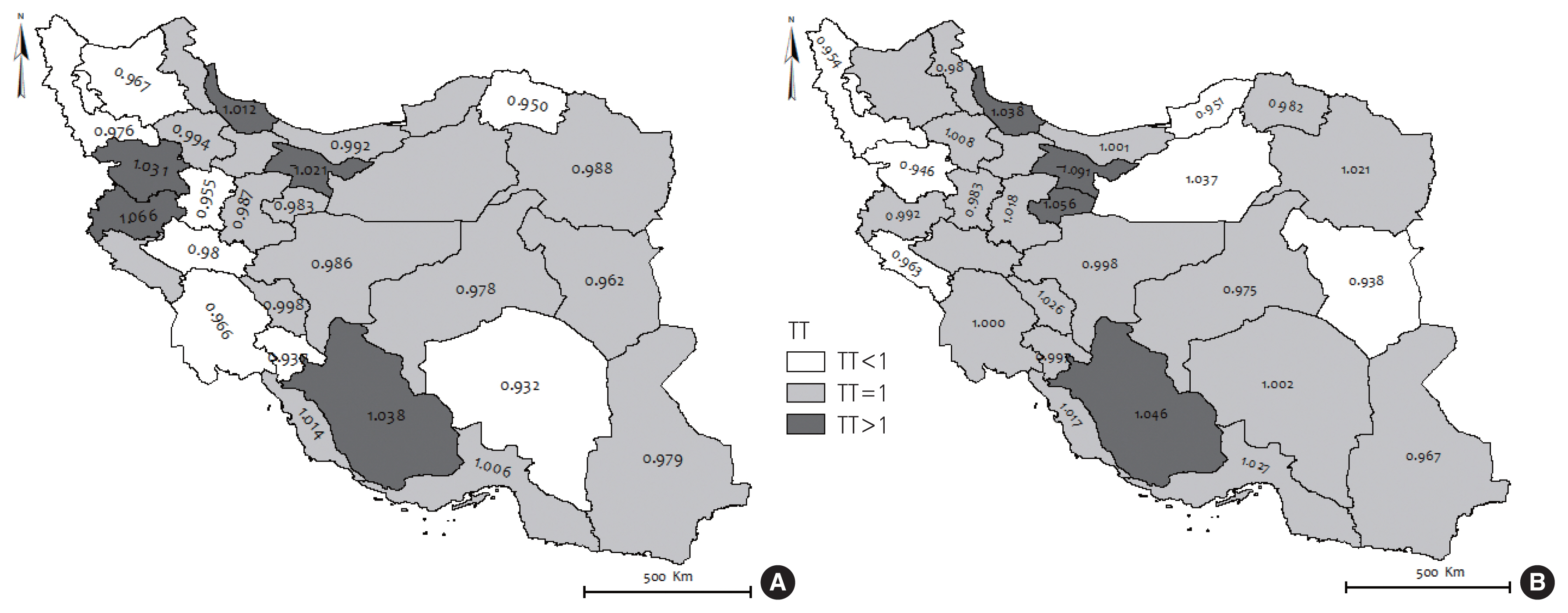
- According to the results of our analysis of TTs, an upward trend in the suicide risk was observed in 5 provinces (16.7%) for men and 4 provinces (13.3%) for women from 2006 to 2016 (Figure 3).
- Suicide Risk by Age
- The 10-year cumulative incidence rates of suicide were 9.96, 5.62, 2.96, and 2.84 deaths per 100 000 population among those aged 15–29 years, 30–49 years, 50–69 years, and >70 years, respectively. According to the BYM model, the nationwide risk of suicide was significantly lower than 1 for those aged 30 years or older, but it was equal to 1 for those aged 15–29. Furthermore, for individuals aged 15–29, 12 provinces (40.0%) had an RR of greater than 1, 5 (16.7%) had an RR equal to 1, and 16 (53.3%) had an RR of less than 1. In addition, 9 (30.0%), 8 (26.7%), and 9 (30.0%) provinces had RRs that were significantly greater than 1 for those aged 30–49 years, 50–69 years, and >70 years, respectively. Among all of the age groups, the highest suicide risk was observed in the provinces of Ilam (P13) and Kermanshah (P15).
- According to the spatio-temporal model, a decreasing pattern of suicide risk was observed for those aged 15–29 (β, −0.006; 95% CrI, −0.010 to −0.0001) and 30–49 (β, −0.001; 95% CrI, −0.018 to −0.002); nonetheless, the trend was stable for individuals aged >50 years.
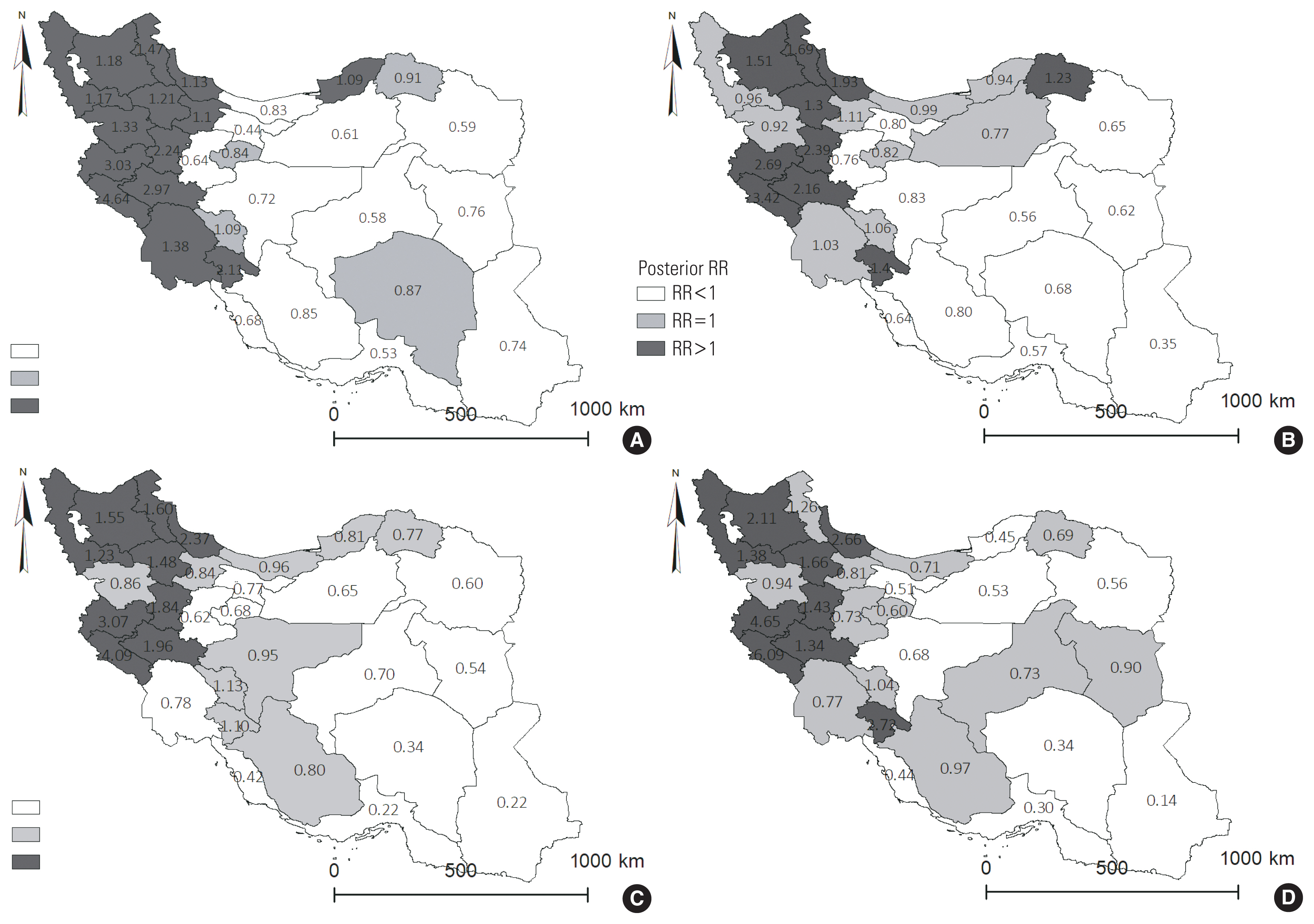
- Figure 4 shows the RR of suicide by age and province. For all age groups, the highest risk of suicide was observed in Iran’s northwestern provinces. Furthermore, upward trends in the suicide risk were observed in the provinces of Fars (P7), Tehran (P28), Hormozgan (P12), Bushehr (P4), and Kermanshah (P15) for individuals aged 15–29 years. Upward trends were also observed in the provinces of Kermanshah (P15) and Fars (P7) for individuals aged 30–49 years. Lastly, upward trends in the suicide risk were observed in the provinces of Kermanshah (P15) and Gilan (P9) for individuals aged 50–69 years and >70 years. Moreover, for all age groups, an RR of greater than 1 and an upward trend in the suicide risk were observed for the province of Kermanshah (P15). The results of the spatio-temporal analysis by province and age are shown in detail in Supplemental Material 1.
- The sensitivity analysis indicated that our main model was consistent with the results of the restricted model used in the sensitivity analysis, which was conducted to determine the robustness of the chosen parameters of the model.
RESULTS
- This is the first epidemiological study on the distribution of the suicide risk in Iran over time at the province level. The results of the present study indicate that the RR of suicide was greater than 1 in 43.0% of Iran’s provinces (PP>0.8) and varied from 0.46 to 3.93. In addition, the results of the spatio-temporal model indicated that the RR of suicide was greater than 1 in 36.7% of provinces, with significant upward TTs observed in Tehran, Fars, Kermanshah, and Gilan; however, the trend was stable for 50.0% of Iran’s provinces. Additionally, the results related to DTs were similar to the results related to TTs. A study by Saberi-Zafaghandi et al. [8] found that the trend in the suicide rate (attempted and successful) increased from 8.3 suicides per 100 000 population in 2001 to 19.4 suicides per 100 000 population in 2005, later declining to 16.3 suicides per 100 000 population in March 2007. The researchers hypothesized that the increase in the suicide rate from 2001 to 2005 was caused by improvements in the system for tracking suicides beginning in 2001, and the decrease in the suicide rate from 2005 to 2007 was attributed to the implementation of suicide prevention programs. Studies from other countries have not shown a uniform trend in the incidence of suicide over the last two decades, and some believe the global suicide rate has decreased in recent years while other studies have shown an increase in the global suicide rate [9–11]. Possible reasons for general increases in the rate of suicide may be related to changes in self-esteem [13], improvements in the system for tracking the number of suicides, the increased prevalence of drug abuse, trends in unemployment, depression, and political issues such as sanctions, economic turmoil, and high inflation [14,15].
- Additionally, the present study showed that, without accounting for TTs, the cumulative incidence of suicide for men and women was 6.75 and 2.88 suicides per 100 000 population, respectively, from 2006 to 2016. According to the results of the BYM model, the cumulative RRs were significantly greater than 1 in 33.3% of Iran’s provinces for women, with the highest RR observed in Ilam (RR, 5.92) followed by Kermanshah (RR, 4.26), Lorestan (RR, 3.65), and Kohkiluyeh-Buyerahmad (RR, 2.03).
- Likewise, the RRs were significantly greater than 1 in 11 (36.4%) of Iran’s provinces for men, with the highest RRs observed in Kermanshah (RR, 3.25), Ilam (RR, 2.98), Hamadan (RR, 2.17), and Lorestan (RR, 2.00) during the 10-year study period. In addition, the spatio-temporal model by gender and province showed a significantly decreasing pattern of risk for men and a stable pattern of risk for women. Our findings indicated a higher risk of suicide among men than among women, which is consistent with the findings of other studies in the same regions [16–18]. There is high variability in the risk factors for suicide in Iran due to regional-level variation in socioeconomic factors, culture, beliefs, family conflict, and cognitive behaviors [14,19]. The province with the lowest reported level of economic prosperity was Ilam, and the highest prevalence of family conflict and depression was observed in Fars and Gilan. To explain the discrepancy in the suicide rate between the genders, men may tend to have a higher degree of determination than women concerning their intention to commit suicide and use methods with high lethality [20]. In addition, in most countries, men are the head of the family and may face more environmental, social, and economic pressures than women. Two studies from Iran by Kiadaliri et al. [19] and Amiri et al. [21] found a ratio of successful suicide of 2.27 among men compared to 2.34 among women. Other studies have suggested that various risk factors for suicide in men and women are among the reasons for this discrepancy. For example, family disputes, chronic illnesses, disabilities, and mental disorders may disproportionately affect men, while family disputes, spousal abuse, mental disorders, and frustration, discouragement, and failure in romantic relationships may play a more influential role in suicide among women [22]. Generally, given the more rapidly rising trend in deaths from suicide among men than among women, it is expected that the discrepancy in suicide deaths between men and women will increase in the future [23,24]. Therefore, preventive and educational care measures for men should be prioritized and implemented.
- According to the BYM model, the nationwide suicide risk was significantly lower than 1 for those older than 30 years of age; however, for those aged 15 to 29, the risk was equal to 1. Furthermore, those aged 15 to 29 had RRs that were greater than 1 in 12 provinces, equal to 1 in 5 provinces, and less than 1 in 16 provinces. Additionally, according to the spatio-temporal model, a decreasing pattern of suicide risk was observed for those aged 15–29 years and 30–49 years; however, the trend was stable for those aged >50 years. These results are consistent with the results of other studies in this field [2,25–27]. A study by Poorolajal et al. [28] found that most suicides were undertaken by individuals younger than 39 years of age and that the incidence of suicide increased with age. A study by Alvaro-Meca et al. [27] found that the suicide mortality rate in Spain was higher for women aged 35–49 years from 1981 to 2008 compared to other age groups. Another study from Estonia found that the highest suicide rate by age was 15–29 years for Asian men and women and 45–59 years old for European men [2]. A study by Rostami et al. [29] reported that the highest number of suicides in Iran were undertaken by individuals aged 20–39 in the province of Kermanshah (Iran). According to several other reports, the age group with the highest rate of attempted suicide and among whom 80% of attempted suicides are undertaken are those aged 15–35 years old, particularly teens and adolescents [30,31]. People in these age groups, especially men, are often responsible for providing living expenses for their families. They also tend to face a higher quantity of other stressors in general, such as marriage, employment, economic hardship, and environmental exposures, than other age groups. Additionally, mental disorders such as depression, schizophrenia, and addiction or substance abuse are more common among this demographic [15,32]. Therefore, the needs of these groups should be especially considered when designing and implementing suicide prevention interventions.
- This study has several limitations. Since this is an ecological study, it was vulnerable to the ecological fallacy. Therefore, determinants of suicide mortality at the national level may not necessarily correlate to determinants at the individual level. In addition, in order to avoid any problematic interpretations or causal inferences, additional studies at the individual level are required.
- We did not include socio-demographic data in our models due to a lack of sufficient information in several of Iran’s provinces. The major strength of this study is that it used longitudinal national databases and statistical methods to accurately estimate the suicide risk in Iran.
- Our study specifically identified regional hotspots and trends in the risk of suicide across Iran’s provinces. The suicide risk differed according to age, gender, and province. It is crucial to allocate resources to address this problem and prevent further depletion of global healthcare resources. Despite the relatively low risk of suicide in the provinces of Tehran, Fars, and Gilan, the rate is increasing rapidly in these provinces compared to other regions. Improving social support by implementing effective plans to manage the factors associated with suicide among Kurdish women and those living in Iran’s northwestern provinces can reduce the number of suicide deaths in Iran.
DISCUSSION
SUPPLEMENTAL MATERIALS
Supplemental Material 1.
ACKNOWLEDGEMENTS
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Conceptualization: Hashemi Nazari SS, Arsang-Jang S. Data curation: Hashemi Nazari SS, Shojaei A, Arsang-Jang S. Formal analysis: Mansori K, Nazari Kangavari H, Arsang-Jang S. Funding acquisition: None. Methodology: Hashemi Nazari SS, Mansori K, Nazari Kangavari H, Shojaei A, Arsang-Jang S. Project administration: Hashemi Nazari SS, Arsang-Jang S. Visualization: Mansori K, Nazari Kangavari H, Arsang-Jang S. Writing – original draft: Hashemi Nazari SS, Mansori K, Nazari Kangavari H, Shojaei A, Arsang-Jang S. Writing – review & editing: Hashemi Nazari SS, Mansori K, Nazari Kangavari H, Shojaei A, Arsang-Jang S.
Notes


- 1. World Health Organization. Preventing suicide: a global imperative; 2014 [cited 2021 Jun 17]. Available from: https://www.who.int/publications/i/item/9789241564779
- 2. Värnik P. Suicide in the world. Int J Environ Res Public Health 2012;9(3):760-771ArticlePubMedPMC
- 3. Crump C, Sundquist K, Sundquist J, Winkleby MA. Sociodemographic, psychiatric and somatic risk factors for suicide: a Swedish national cohort study. Psychol Med 2014;44(2):279-289ArticlePubMed
- 4. Qi X, Tong S, Hu W. Preliminary spatiotemporal analysis of the association between socio-environmental factors and suicide. Environ Health 2009;8: 46ArticlePubMedPMC
- 5. Likhvar V, Honda Y, Ono M. Relation between temperature and suicide mortality in Japan in the presence of other confounding factors using time-series analysis with a semiparametric approach. Environ Health Prev Med 2011;16(1):36-43ArticlePubMed
- 6. Qi X, Hu W, Page A, Tong S. Associations between climate variability, unemployment and suicide in Australia: a multicity study. BMC Psychiatry 2015;15: 114ArticlePubMedPMC
- 7. Fazel S, Grann M, Kling B, Hawton K. Prison suicide in 12 countries: an ecological study of 861 suicides during 2003–2007. Soc Psychiatry Psychiatr Epidemiol 2011;46(3):191-195ArticlePubMed
- 8. Saberi-Zafaghandi MB, Hajebi A, Eskandarieh S, Ahmadzad-Asl M. Epidemiology of suicide and attempted suicide derived from the health system database in the Islamic Republic of Iran: 2001–2007. East Mediterr Health J 2012;18(8):836-841ArticlePubMed
- 9. Kessler RC, Berglund P, Borges G, Nock M, Wang PS. Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990–1992 to 2001–2003. JAMA 2005;293(20):2487-2495ArticlePubMed
- 10. Largey M, Kelly CB, Stevenson M. A study of suicide rates in Northern Ireland 1984–2002. Ulster Med J 2009;78(1):16-20PubMedPMC
- 11. Isacsson G, Holmgren A, Osby U, Ahlner J. Decrease in suicide among the individuals treated with antidepressants: a controlled study of antidepressants in suicide, Sweden 1995–2005. Acta Psychiatr Scand 2009;120(1):37-44ArticlePubMed
- 12. Abellan JJ, Richardson S, Best N. Use of space-time models to investigate the stability of patterns of disease. Environ Health Perspect 2008;116(8):1111-1119ArticlePubMedPMC
- 13. Choi YS, Shin HK, Hong DY, Kim JR, Kang YS, Jeong B, et al. Self-esteem as a moderator of the effects of happiness, depression, and hostility on suicidality among early adolescents in Korea. J Prev Med Public Health 2019;52(1):30-40ArticlePubMedPMC
- 14. Nazarzadeh M, Bidel Z, Ayubi E, Soori H, Sayehmiri K. Factors related to suicide attempt in Iran: a systematic review and meta-analysis. Hakim Res J 2013;15(4):352-363. (Persian)
- 15. Janghorbani M, Sharifirad GR. Completed and attempted suicide in Ilam, Iran (1995–2002): incidence and associated factors. Arch Iranian Med 2005;8(2):119-126
- 16. Zarenezhad M, Gorgi Z, SheikhFathollahi M, Gholamzadeh S, Ghadipasha M, Rezaeian M. Epidemiological survey of suicide in Fars Province in the south of Iran during 2003 to 2011. J Rafsanjan Univ Med Sci 2015;13(12):1129-1140. (Persian)
- 17. Thomas K, Gunnell D. Suicide in England and Wales 1861–2007: a time-trends analysis. Int J Epidemiol 2010;39(6):1464-1475ArticlePubMed
- 18. Najafi F, Hasanzadeh J, Moradinazar M, Faramarzi H, Nematollahi A. An epidemiological survey of the suicide incidence trends in the southwest Iran: 2004–2009. Int J Health Policy Manag 2013;1(3):219-222ArticlePubMedPMC
- 19. Kiadaliri AA, Saadat S, Shahnavazi H, Haghparast-Bidgoli H. Overall, gender and social inequalities in suicide mortality in Iran, 2006–2010: a time trend province-level study. BMJ Open 2014;4(8):e005227ArticlePubMedPMC
- 20. khazaei S, karami M, Sohailzade M, Sohrabnegad A. Determinants of complete suicide: a cross sectional study. J Ilam Univ Med Sci 2013;21(6):240-247. (Persian)
- 21. Amiri B, Pourreza A, Rahimi Foroushani A, Hosseini SM, Poorolajal J. Suicide and associated risk factors in Hamadan province, west of Iran, in 2008 and 2009. J Res Health Sci 2012;12(2):88-92PubMed
- 22. Balasooriya NN, Kularathne MG. Trends of risk factors of completed suicide by gender and age. J Public Health Epidemiol 2016;8(7):115-120Article
- 23. Skinner R, McFaull S, Draca J, Frechette M, Kaur J, Pearson C, et al. Suicide and self-inflicted injury hospitalizations in Canada (1979 to 2014/15). Health Promot Chronic Dis Prev Can 2016;36(11):243-251ArticlePubMedPMC
- 24. Patel V, Ramasundarahettige C, Vijayakumar L, Thakur JS, Gajalakshmi V, Gururaj G, et al. Suicide mortality in India: a nationally representative survey. Lancet 2012;379(9834):2343-2351ArticlePubMedPMC
- 25. Wasserman D, Cheng Q, Jiang GX. Global suicide rates among young people aged 15–19. World Psychiatry 2005;4(2):114-120PubMedPMC
- 26. Bridge JA, Goldstein TR, Brent DA. Adolescent suicide and suicidal behavior. J Child Psychol Psychiatry 2006;47(3–4):372-394ArticlePubMed
- 27. Alvaro-Meca A, Kneib T, Gil-Prieto R, Gil de Miguel A. Epidemiology of suicide in Spain, 1981–2008: a spatiotemporal analysis. Public Health 2013;127(4):380-385ArticlePubMed
- 28. Poorolajal J, Rostami M, Mahjub H, Esmailnasab N. Completed suicide and associated risk factors: a six-year population based survey. Arch Iran Med 2015;18(1):39-43PubMed
- 29. Rostami M, Jalilian A, Rezaei-Zangeneh R, Salari A. Factors associated with the choice of suicide method in Kermanshah Province, Iran. Ann Saudi Med 2016;36(1):7-16ArticlePubMedPMC
- 30. Spicer RS, Miller TR. Suicide acts in 8 states: incidence and case fatality rates by demographics and method. Am J Public Health 2000;90(12):1885-1891ArticlePubMedPMC
- 31. Erlangsen A, Bille-Brahe U, Jeune B. Differences in suicide between the old and the oldest old. J Gerontol B Psychol Sci Soc Sci 2003;58(5):S314-S322ArticlePubMed
- 32. Bae HC, Hong S, Jang SI, Lee KS, Park EC. Patterns of alcohol consumption and suicidal behavior: findings from the fourth and fifth Korea National Health and Nutritional Examination Survey (2007–2011). J Prev Med Public Health 2015;48(3):142-150ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Spatial, geographic, and demographic factors associated with adolescent and youth suicide: a systematic review study
Masoud Ghadipasha, Ramin Talaie, Zohreh Mahmoodi, Salah Eddin Karimi, Mehdi Forouzesh, Masoud Morsalpour, Seyed Amirhosein Mahdavi, Seyed Shahram Mousavi, Shayesteh Ashrafiesfahani, Roya Kordrostami, Nahid Dadashzadehasl
Frontiers in Psychiatry.2024;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite