Factors Affecting Breast Self-examination Behavior Among Female Healthcare Workers in Iran: The Role of Social Support Theory
Article information

Abstract
Objectives
In women, breast cancer is the most common cancer and the leading cause of cancer death. Screening tests are the basis for early diagnosis. In Iranian women, the mortality rate of breast cancer is high due to insufficient screening examinations and delayed visits for care. Therefore, this study aimed to determine the factors affecting breast self-examinations among Iranian women employed in medical careers.
Methods
This cross-sectional study included 501 women working in the medical professions at Hamadan University of Medical Sciences in western Iran in 2018. The subjects were selected by stratified random sampling. Data were collected using a researcher-developed, self-report questionnaire that contained demographic information and questions based on protection motivation theory and social support theory. Descriptive data analysis was conducted using SPSS version 23 and model fitting with PLS version 2.
Results
The mean age of the participants was 37.1±8.3 years, and most of the women (80.4%) were married. Most women had a bachelor’s degree (67.5%). The findings of this study showed that the coping appraisal construct was a predictor of protection motivation (β=0.380, p<0.05), and protection motivation (β=0.604, p<0.05) was a predictor of breast self-examination behavior. Additionally, social support theory (β=0.202, p<0.05) had a significant positive effect on breast self-examination behavior.
Conclusions
The frequency of practicing self-examinations among women employees in the medical sector was low; considering the influence of social support as a factor promoting screening, it is necessary to pay attention to influential people in women’s lives when designing educational interventions.
INTRODUCTION
Breast cancer is the most common form of cancer among women and the leading cause of cancer death among women in many countries [1]. In Iran, breast cancer is likewise the most common cancer among women [2]. Breast cancer leads to various physical, psychological, social, economic, and familial problems; it reduces self-esteem and increases patients’ sense of vulnerability, pain, and absence from work [3]. Breast cancer is a major health problem for Iranian women, because most women are never screened. Therefore, breast cancer is generally diagnosed very late [4]. Early diagnosis of breast cancer is a potentially beneficial way to control the disease and to reduce mortality. Annual mammography, clinical breast examinations, and monthly breast self-examinations (BSEs) are essential for the early diagnosis of breast cancer [1]. BSEs, which are performed by touching the breast with the finger tips, are done in order to find masses. Through this method, women can check their breasts in sitting, standing, or lying positions. BSEs are routinely carried out in advanced countries, but are often not considered to be appropriate in developing countries [5]. Perceived barriers prevent screening, including the absence of signs and concerns about lack of recognition [6]; fear [7]; lack of doctors’ recommendations, forgetting the schedule of BSEs, pain, and embarrassment [8]; lack of environmental support and cultural beliefs about fate [9]; and the absence of support from spouse, friends, and family [10]. Studies have shown that existence of social support increases women’s participation in breast cancer screening programs [10-13]. Social support is categorized into 4 categories. Emotional support includes empathy, love, trust, and care. Instrumental support refers to tangible assistance. Informational support manifests as advice, comments, and information that a person can use in the face of a problem. Appraisal support refers to the provision of information that is useful for internal evaluation [14].
In this study, protection motivation theory (PMT) was used as a theoretical framework for identifying factors affecting whether Iranian employed women perform BSEs. This model suggests that protection motivation (i.e., the intention to engage in protective behavior) is derived from the 2 processes of threat appraisal and coping appraisal. The effective variables in this model include susceptibility construct, severity construct, response efficacy, self-efficacy, rewards associated with incompatible responses, and response costs of consistent behavior. PMT is used as a cognitive social model to predict various behaviors, such as cancer screening. However, a limitation of PMT is that it cannot detect environmental and cognitive variables (such as subjective norms) that affect behavior change [15,16]. Therefore, the main purpose of this study was to answer the following question: does the social support theory resolve this weakness of PMT? (Supplemental Material 1).
METHODS
In this cross-sectional study, the participants were 501 women working in the medical professions at Hamadan University of Medical Sciences in western Iran in 2018. Since the total number of employed women in the Medical Sciences University units was 3030, and previous studies have reported different levels of prevalence of BSEs, in order to determine the sample size, a rate of 73% [17] with an alpha value of 0.01, accuracy of 0.05, and confidence level of 99% were considered. Finally, after taking into account a 10% projected loss to follow-up, 501 employed women were enrolled in the study. After obtaining approval from Hamadan University of Medical Sciences and receiving a list of employees, the names of individuals in the research units were selected through multi-stage sampling (stratified random sampling). Considering that Hamadan University of Medical Sciences has educational, health, medical, and office units, at first, the number and names of employed people, as well as the actual percentage of individuals to be sampled in each unit, were obtained. Then, the women’s names in each unit were separately entered into the Research Randomizer (https://www.randomizer.org/), and the number of individuals to be sampled in each unit was determined randomly. The researchers went to the relevant location and presented the questionnaire to the selected subjects to complete. If the selected subjects did not choose to participate in the study or were not present when there searchers was there, alternative subjects were re-selected using the software. The inclusion criteria for participation in the study were consent and willingness to participate in the study, age between 20 years to 61 years, and the lack of a history of breast cancer. The exclusion criteria were having breast cancer at the time of the study and incomplete completion of the questionnaire. The tool used to collect information was a researcher-developed questionnaire consisting of 3 sections on demographic information (Table 1), the PMT constructs, and the theoretical construct of social support [18-22].
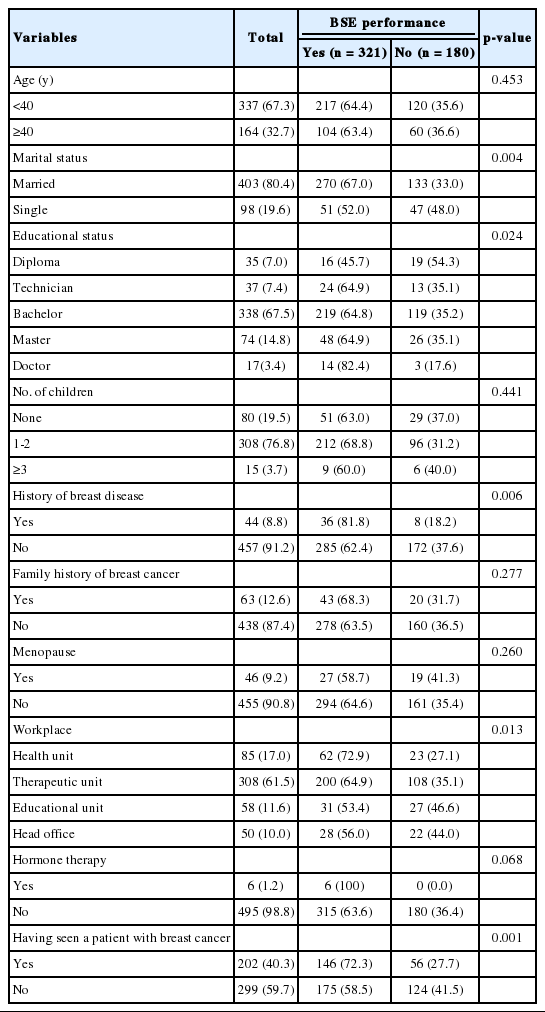
Relationships between demographic variables and breast self-examination (BSE) performance (n=501)
The part of the questionnaire dealing with the PMT constructs contained questions on a 5-point Likert scale, arranged as follows: 8 questions on the severity construct, 6 questions on the self-efficacy construct, 7 questions on the response efficacy construct, 4 questions on the response costs construct, 5 questions on the reward construct, 4 questions on the fear construct, and 4 questions on the protection motivation construct. The part of the questionnaire dealing with social support likewise consisted of questions on a 5-point Likert scale, distributed as follows: 5 questions on the emotional support construct, 3 questions on the informational support construct, 3 questions on the instrumental support construct, and 3 questions on the appraisal support construct. In more detail, the 5-point Likert scale was constructed with scores of 1-5 assigned to responses of “I completely disagree,” “I disagree,” “I have no idea,” “I agree,” and “I completely agree.” The scoring of answers to questions about the response costs construct and the reward construct was reversed. The domains of the scores and questions are presented in Table 2. To determine the content validity of the questionnaire, 10 questionnaires were distributed to specialists in health education, gynecology, and oncology. To evaluate content validity, the content validity ratio (CVR) and content validity index (CVI) were used. A CVI score of 0.7 or higher and a CVR score of 0.6 or above were considered acceptable (Table 3) [16,23]. To determine the formal validity of the questions, 10 women were asked to give their opinion about the simplicity, clarity, and readability of questions. Vague questions were revised.
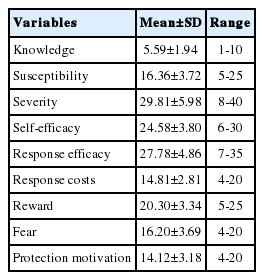
Mean, standard deviation (SD), and range of scores for the constructs of protection motivation theory (n=501)
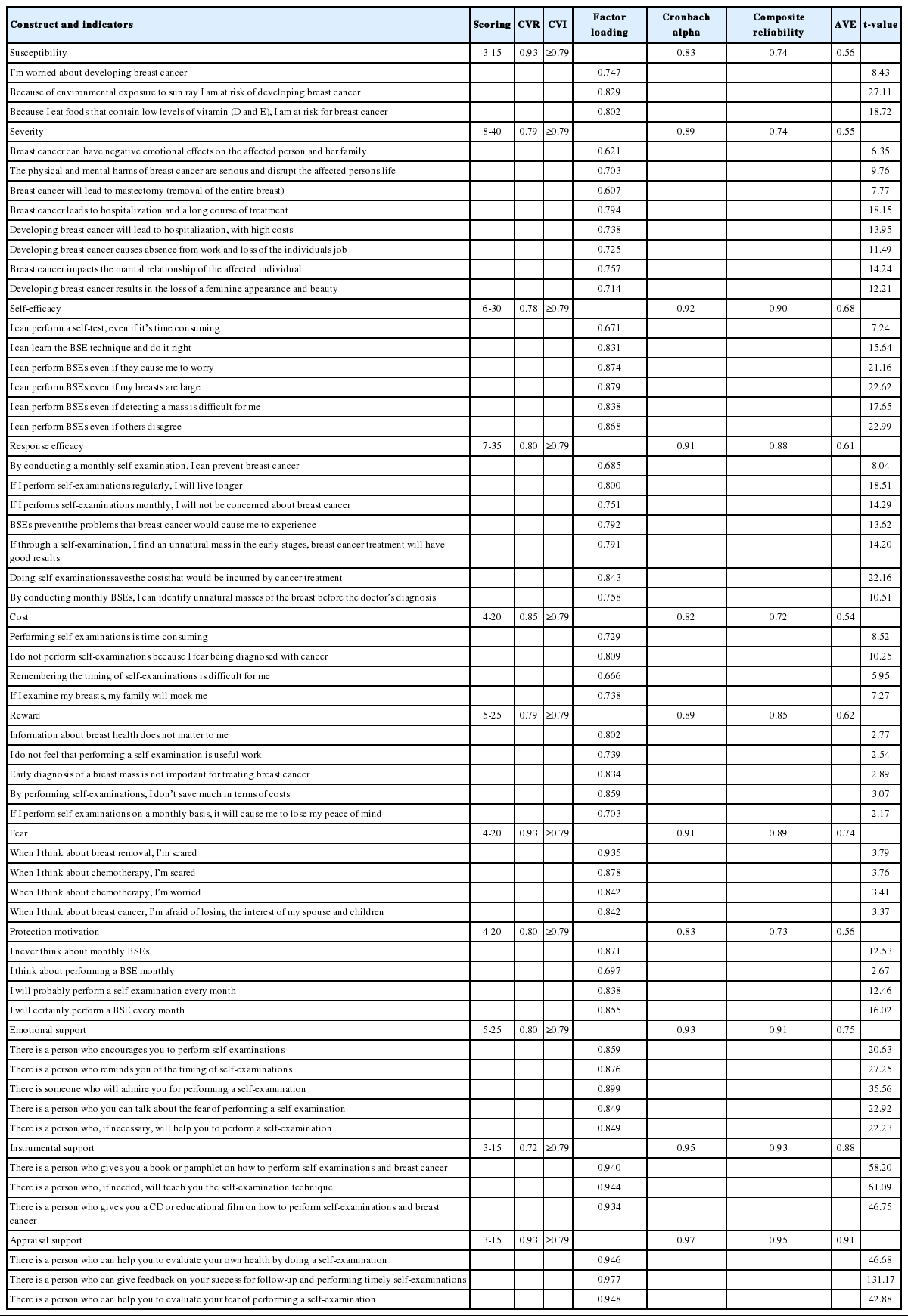
Validity of the questionnaire and measurement model indices
Exploratory factor analysis was used for construct validity, which was calculated for all samples (501 individuals). In order to conduct factor analysis, first, the adequacy of the sample size was confirmed using the Kaiser–Meyer–Olkin (KMO) measure, and for correlations between measured variables, the Bartlett test of sphericity was used. Acceptable KMO values range from 0.7 to 0.8 [24]. In our study, the KMO statistic was 0.75, indicating that the sample was suitable for performing factor analysis. The null assumption of the Bartlett test of sphericityis that variables correlate only with themselves. Therefore, rejection of this assumption shows the suitability of the correlation matrix for factor analysis [25]. In other words, the items are correlated with each other. In this analysis, the varimax rotation method was selected to achieve the best factor loading (>0.4) [25,26].
To assess the reliability of the tool, internal consistency and re-testing were used. To measure internal consistency, a pilot study was conducted among 30 women employed at Hamadan University of Medical Sciences. Cronbach alpha coefficients above 0.70 were considered acceptable, and the Cronbach alpha was calculated to be 0.83. To calculate the reliability by the re-test method, the questionnaire was filled out by 30 participants and then the subjects completed the questionnaires for a second time within 2 weeks. An intraclass correlation coefficient (ICC) value of 0.80 or higher shows high reliability, an ICC value between 0.60 and 0.79 shows moderate reliability, and an ICC value less than 0.60 shows poor reliability [27]. In the present study, the ICC was 0.99.
Data Analysis
The results of this study were analyzed using SPSS version 23 (IBM Corp., Armonk, NY, USA) and structural equation modeling (SEM) with PLS version 2 (SmartPLS GmbH, Bönningstedt, Germany). SEM is an approach that consists of 2 stages: a measuring model and a structural model [28].
Measurement Model
To investigate the fit of the measuring models, the 3 criteria of reliability, convergent validity, and divergent validity were used.
In this step, to examine the questions’ homogeneity, their factor loadings and t-values were evaluated. The measurement of factor loadings utilized a threshold of ≥0.4, and significant t-values were considered to be >96.1. In the present study, due to low factor loadings, the first and second questions of the susceptibility construct were removed. In the next step, to examine the reliability of the instrument, composite reliability was assessed using the Cronbach alpha with acceptable threshold of >0.7, and the average extracted mean variance (AVE criterion) was used to assess convergent validity, using a threshold of >0.5 [29,30].
After confirming the homogeneity and reliability of the instrument, divergent validity was investigated. This refers to the concept that the questions measuring some variables should be different from those measuring other variables. Divergent validity was evaluated using the Fornell-Larcker method [30].
Once suitable measurement indicators were confirmed, the analysis proceeded to the structural model step.
Ethics Statement
This study was approved by the Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1396.609). The researcher also pledged to keep all information confidential. Participation in this study was voluntary, and the participants could discontinue participation at any time and for any reason.
RESULTS
In this study, the participation rate was 100%.
Descriptive Statistics
The majority of the studied population (67.3%) were under 40 years old, and most participants (80.4%) were married. Most participants had a bachelor’s degree (67.5%), 91.2% had no personal history of breast disease, and 87.4% had no family history of breast cancer. Only 9% of the subjects performed monthly BSEs on a regular basis. The relationships between demographic variables and BSE behavior are presented in Table 1. In the present study, respondents had low scores for their level of knowledge and for the various constructs of PMT. The mean, standard deviation, and range of scores for the PMT constructs are presented in Table 2.
Measurement Model
The results showed that the factor loading of each item for its variable was greater than its factor loading for the remaining variables. Therefore, divergent validity was confirmed (Table 3).
Structural Model
Based on the results of the path analysis, the protection motivation construct (β=0.890, p<0.05) and social support (β=0.202, p<0.05) had significant relationships with BSE behavior. However, social support (β=0.020, p>0.05) did not have a significant relationship with intentions. A significant relationship was found between response costs and coping appraisal (β=0342, p<0.05). Coping appraisal showed significant relationships with self-efficacy (β=0.900, p<0.05), response efficacy (β=0.892, p<0.05), and the protection motivation construct (β=0.380, p<0.05). Threat appraisal showed significant relationships with severity (β=0.948, p<0.05) and susceptibility (β=0.638, p<0.05). Furthermore, social support showed significant relationships with emotional support (β=0.791, p<0.05), information support (β=0.889, p<0.05), instrumental support (β=0.804, p<0.05), and appraisal support (β=0.890, p<0.05). Non-significant relationships were found between the threat appraisal construct and the protection motivation construct (β=0.091), the threat appraisal construct and the reward construct (β=0.067), and the fear construct and protection motivation (β=-0.154) (Table 4).
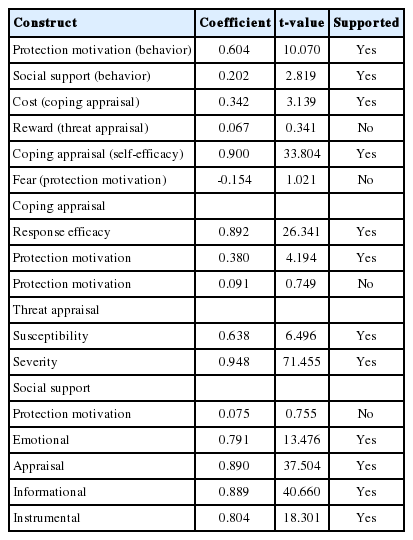
Results of indicators and structural model criteria
Social support had a positive and significant effect on BSE behavior and had no effect on protection motivation. No evidence of fit was found for these results (Figure 1). Finally, the goodness-of-fit (GOF) of the final model was evaluated. Wetzels et al. [31] suggested that GOF values above 0.36 indicate that the model is suitable for behavioral science. In the present study, the GOF model was estimated to be 0.60.
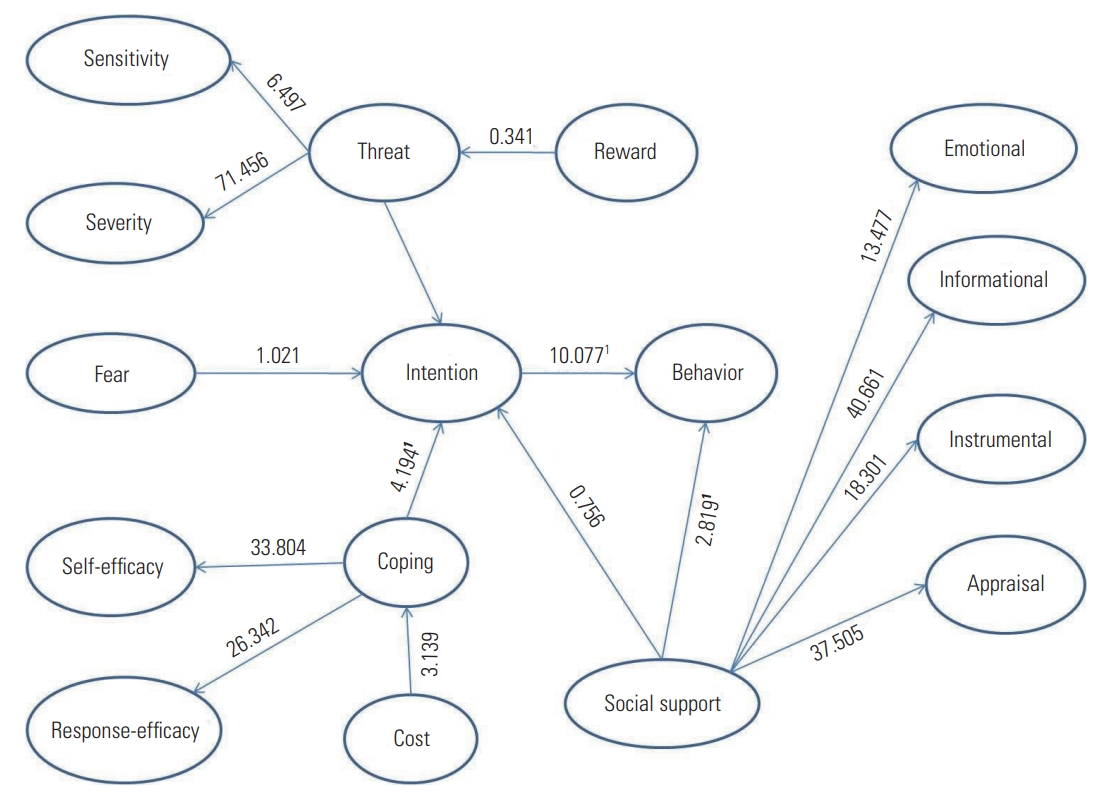
Motivation theory with social support theory based on t-values. To test the hypotheses, structural equation modeling was used from t-values. If the magnitude of the absolute value is greater than 96/1, it indicates that the relationship between the structures is correct and, therefore, confirms the research hypotheses at 95% confidence level. 1t-value.
DISCUSSION
The purpose of this study was to develop PMT through the use of social support theory. Suitable fitting of the model was observed. In the present study, the proportion of respondents employed in the medical professions who regularly conducted BSEs was found to be low, which is consistent with previous studies [32-34]. In this research, our main hypothesis was that factors identified in social support theory would influence the protection motivation construct of BSE. The hypothesis test showed that social support had a positive and significant effect on BSE behavior, but no effect on protection motivation. No evidence of fit was found for these results. However, this finding does imply that social support from colleagues, friends, and family members has an impact on information access, individual encouragement, and the adoption of preventive behaviors. By increasing self-efficacy, social support helps individuals overcome perceived barriers (emotional, logical, and financial) to breast cancer screening [11]. Therefore, when designing educational programs, is essential to pay attention to the role of influential people in individuals’ daily lives.
In some studies, such as those conducted by Farhadifar et al. [11] and Messina et al. [35], social support positively influenced protection motivation for screening, which is not consistent with the present study.
Another result of this study is that coping appraisal was found to be the strongest predictor of protection motivation for screening behavior, similar to results reported in other studies [15,16]. Therefore, considering self-efficacy and the response efficacy construct, which are components of coping appraisal, can improve the degree to which individuals engage in screening behavior.
The findings of this study showed that there was a correlation between the response cost and coping appraisal. This means that higher costs of consistent behaviors can be a barrier to engaging in those behaviors, resulting in reduced self-efficacy. In this study, it was also found that there was no significant relationship between the fear construct and the protection motivation construct, in contrast to the study conducted by Helmes [36]. Fear is a barrier to screening behavior. The study conducted by Ackerson and Preston [37] obtained a similar result to that of the present study. Therefore, identifying and removing behavioral barriers may help to increase consistent behaviors.
Another noteworthy finding of this study was the presence of significant relationships between coping appraisal and the susceptibility and severity constructs. According to PMT, coping appraisal consists of a combination of the 2 constructs of susceptibility and severity [38].
Greater perceived susceptibility regarding the possibility of developing breast cancer results in increased screening behaviors. The severity construct refers to the concept that the frequency of preventive behaviors will increase in correspondence with an individual’s mental beliefs about the disease and the disadvantages posed by its complications [15]. Therefore, the greater the perceived threat, the more common screening behavior will be. This result is consistent with the findings of Barati et al. [39]. For this reason, when designing educational programs, attention should be paid to the characteristics of the community and, by promoting threat appraisal, people should be encouraged to reach the risk control stage.
In the present study, no significant relationship was observed between the threat appraisal construct and the protection motivation construct. This finding is not consistent with the results of the studies of Barati et al. [39] and Yan et al. [40]. When a threat is not taken seriously (low severity), individuals have a low motivation to evaluate the effectiveness of the recommended solutions. Those who believe that the threat is serious and are endangered by its negative consequences have a greater motivation to protect themselves.
The present study had limitations. First, BSEs are no longer recommended by the American Cancer Society. However, one of the most important reasons for regular BSEs is that they enable women to know what is normal for their breasts so that they can identify any changes, which is critical to managing their breast health. If women see or feel something different or unusual while performing a BSE, they should see their doctor without delay. Second, the results cannot be generalized to all employed women in all environments, because the information was collected exclusively from medical professionals at Hamadan University of Medical Sciences. Third, the information was self-reported.
In conclusion, the frequency of regular BSEs in Iranian employed women was low. Considering the influence of social support as a factor promoting regular screening, it is necessary to pay attention to influential people in women’s daily life when designing educational interventions.
The components of social support theory play an important role in empowering women. These factors, including emotional support (patient communication with a physician or support from family/friends) and information support (educational materials) should be applied to improve breast cancer screening, which will reduce fear and promote self-efficacy.
SUPPLEMENTAL MATERIALS
Supplemental material is available at https://doi.org/10.3961/jpmph.18.277.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
ACKNOWLEDGEMENTS
This article is part of a Ph.D. dissertation in Health Education and Health Promotion at Hamadan University of Medical Sciences. We thank the individuals who participated in this project.
This work was financially supported by Hamadan University of Medical Sciences (grant No. 9603091553).
Notes
AUTHOR CONTRIBUTIONS
Conceptualization: SB. Data curation: MD. Formal analysis: YM, MD. Funding acquisition: SB. Methodology: SB, MB, LMS. Project administration: SB. Visualization: SB, MB. Writing - original draft: MD. Writing - review & editing: MD, SB, MB, LMS, YM.