Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 54(2); 2021 > Article
-
Systematic Review
Prevalence of Sarcopenia Among the Elderly in Korea: A Meta-Analysis -
Yoo Jin Choo
 , Min Cheol Chang
, Min Cheol Chang -
Journal of Preventive Medicine and Public Health 2021;54(2):96-102.
DOI: https://doi.org/10.3961/jpmph.21.046
Published online: March 4, 2021
Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, Daegu, Korea
- Corresponding author: Min Cheol Chang Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea E-mail: wheel633@gmail.com
Copyright © 2021 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- Sarcopenia is a common disease in the elderly population that causes disability, poor quality of life, and a high risk of death. In the current study, we conducted a meta-analysis to report basic knowledge about the prevalence of sarcopenia in the elderly in Korea.
-
Methods
- We searched for articles in the MEDLINE, Cochrane Library, Embase, and Scopus databases published until December 28, 2020. Studies investigating the prevalence of sarcopenia in elderly Koreans aged ≥65 years were included. The methodological quality of the studies was evaluated using the Newcastle-Ottawa scale. Publication bias was evaluated using the Egger test and funnel plots.
-
Results
- In total, 3 studies and 2922 patients were included in the meta-analysis. All 3 studies used the European Working Group on Sarcopenia in Older People criteria for the diagnosis of sarcopenia. The total prevalence of sarcopenia was 13.1-14.9% in elderly men and 11.4% in elderly women.
-
Conclusions
- This meta-analysis is the first to estimate the pooled prevalence of sarcopenia in elderly Koreans, and its findings suggest that sarcopenia is common in this population. Therefore, attention should be paid to the prevention and control of sarcopenia.
- Sarcopenia refers to a condition wherein the body’s muscle mass and strength are abnormally decreased or weakened [1]. It is an age-related disease. In general, 1-2% of muscle is lost every year starting at the age of 50 years [2]. In older people, sarcopenia is a major problem that causes disability, poor quality of life, and a high risk of death [3]. In Korea, the prevalence of sarcopenia is increasing because of the increase in the elderly population and life expectancy [4].
- As clinicians’ and researchers’ interest in sarcopenia has increased, several studies have investigated its prevalence [5-7]. However, the prevalence of sarcopenia has been inconsistent in different studies, and no large-scale epidemiological study of sarcopenia has yet been carried out in Korea.
- In the current study, we conducted a meta-analysis and systematically evaluated the prevalence of sarcopenia in elderly Koreans to construct basic data on the prevalence of sarcopenia in Korea.
INTRODUCTION
- Search Strategy
- This meta-analysis was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines [8]. We systematically searched for relevant articles in the PubMed, Embase, Cochrane Library, and Scopus databases for studies published up to December 28, 2020. The following keywords were used in the search: (sarcopenia OR muscle mass OR muscle strength) AND (prevalence OR epidemiology OR frequency OR incidence) AND (Korea).
- Study Selection
- We applied the following inclusion criteria for the selection of articles: (1) the prevalence rate of sarcopenia was evaluated, (2) the study was conducted among Koreans, (3) age of the included subjects was ≥65 years, and (4) loss of appendicular muscle mass and functional decline were considered for the diagnosis of sarcopenia. The exclusion criteria were (1) the same data published repeatedly, and (2) not reporting study outcomes.
- Data Extraction
- After discarding duplicate studies, 2 reviewers (YJC and MCC) independently evaluated the potentially eligible studies. The articles were screened for eligibility by reviewing the title and abstract. Disagreements were resolved through consensus. After screening, the full texts of the eligible articles were read independently by both reviewers, and the eligibility of each article was re-assessed. Subsequently, data on the first author, publication date, study type, number of patients, and demographic characteristics (age, gender, and other participant details) were extracted.
- Quality Assessment
- The Newcastle-Ottawa scale (NOS) for cross-sectional studies was used for quality assessment [9], with 3 aspects (selection, comparability, and outcomes). The judgment of bias was expressed as “unsatisfactory,” “satisfactory,” “good,” or “very good.” The quality of each study was graded as unsatisfactory (0-4), satisfactory (5-6), good (7-8), or very good (9-10). All differences of opinion were resolved by consensus.
- Statistical Analysis
- Using the Comprehensive Meta-Analysis version 2 (Biostat Inc., Englewood, NJ, USA), the extracted data were analyzed using statistical tests. For each analysis, a heterogeneity test was conducted using the I2 statistic to evaluate the extent of inconsistency in the obtained results. If the I2 value was >50%, the data were considered to have substantial heterogeneity, and a random-effects model was used for data analysis. In contrast, if the I2 value was ≤50%, then the pooled data were considered homogeneous and a fixed-effects model was applied for data analysis. The pooled prevalence and 95% confidence interval (CI) of sarcopenia were also calculated.
- Ethics Statement
- Ethical approval was waived because this was a meta-analysis based on previously published studies.
METHODS
- Study Selection
- In total, 721 potentially relevant studies were selected in the preliminary search of all the databases (Figure 1). We excluded 224 duplicate studies and excluded an additional 481 publications after their titles and abstracts were reviewed. The remaining studies were assessed through a review of the full texts of the articles. As a result of full-text screening, 3 articles were included (Table 1) [10-12]. In all 3 articles, the European Working Group on Sarcopenia in Older People (EWGSOP) criteria [13] were used for the diagnosis of sarcopenia.
- Study Characteristics
- The selected studies included 2922 patients (male-to-female ratio, 1455:1467). The characteristics of the selected studies are summarized in Table 1.
- Risk of Bias
- All the included studies were rated 5 points (selection: 2 points; outcome: 3 points). Therefore, the quality of the 3 studies assessed using the NOS was considered satisfactory.
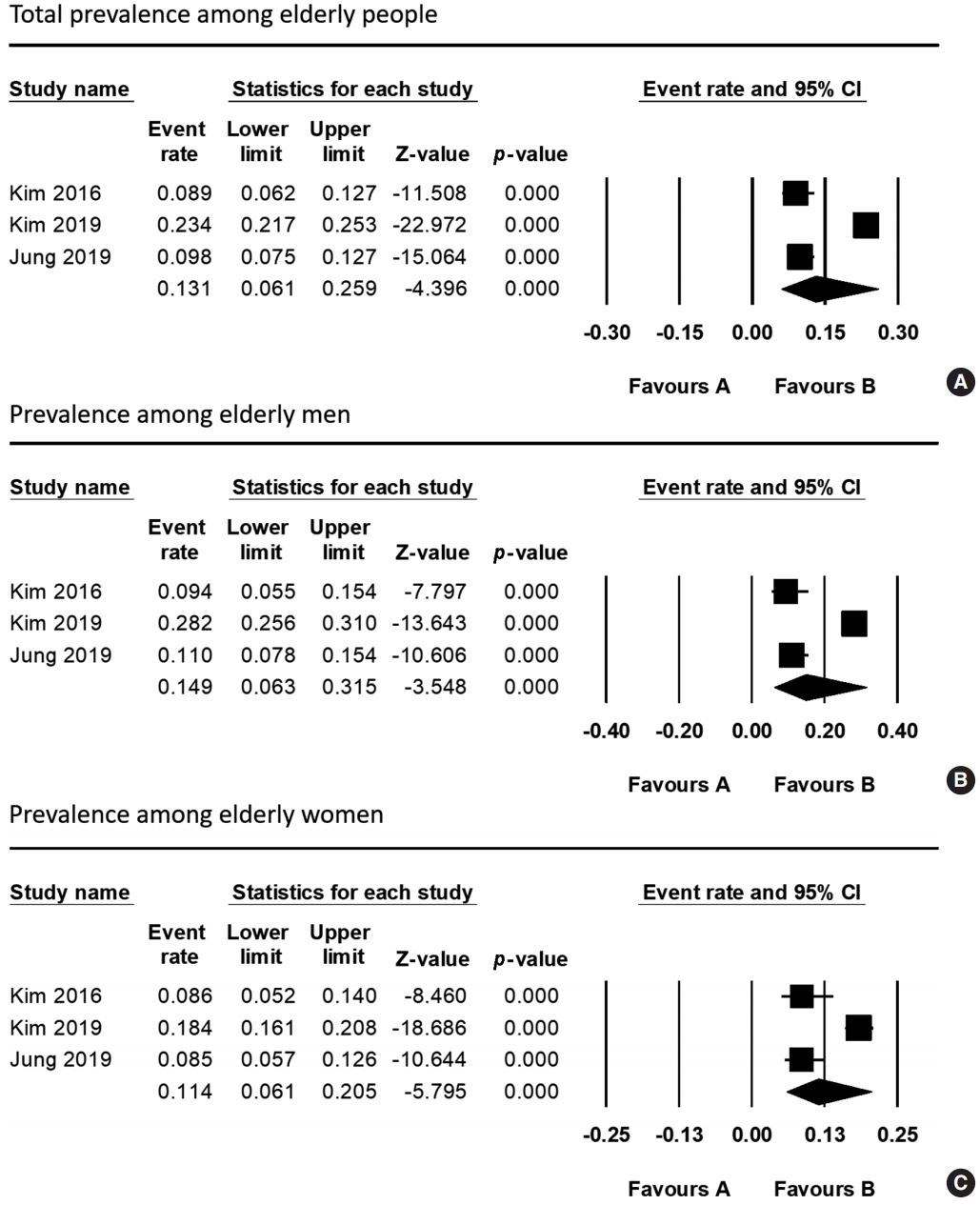
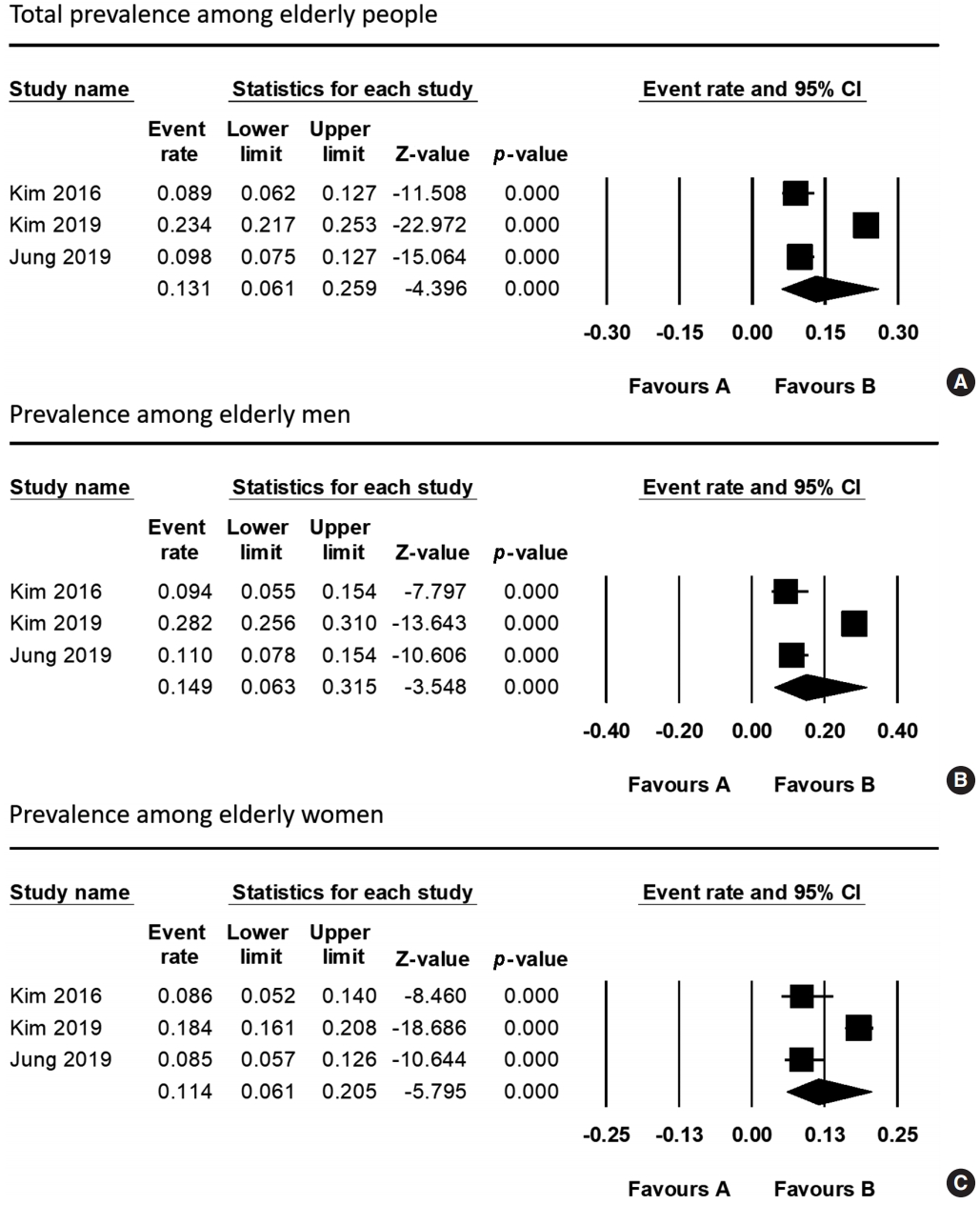
- Meta-analysis Results
- To analyze the prevalence, a random-effects model was used (I2 for total prevalence among elderly people, 97.1%; for prevalence among elderly men, 95.8%; and for prevalence among elderly women, 90.4%). The total prevalence of sarcopenia among elderly Koreans aged ≥65 years was 13.1% (95% CI, 6.1 to 25.9) (Figure 2). The prevalence of sarcopenia among elderly Korean men was 14.9% (95% CI, 6.3 to 31.5), whereas the prevalence of sarcopenia among elderly Korean women was 11.4% (95% CI, 6.1 to 20.5).
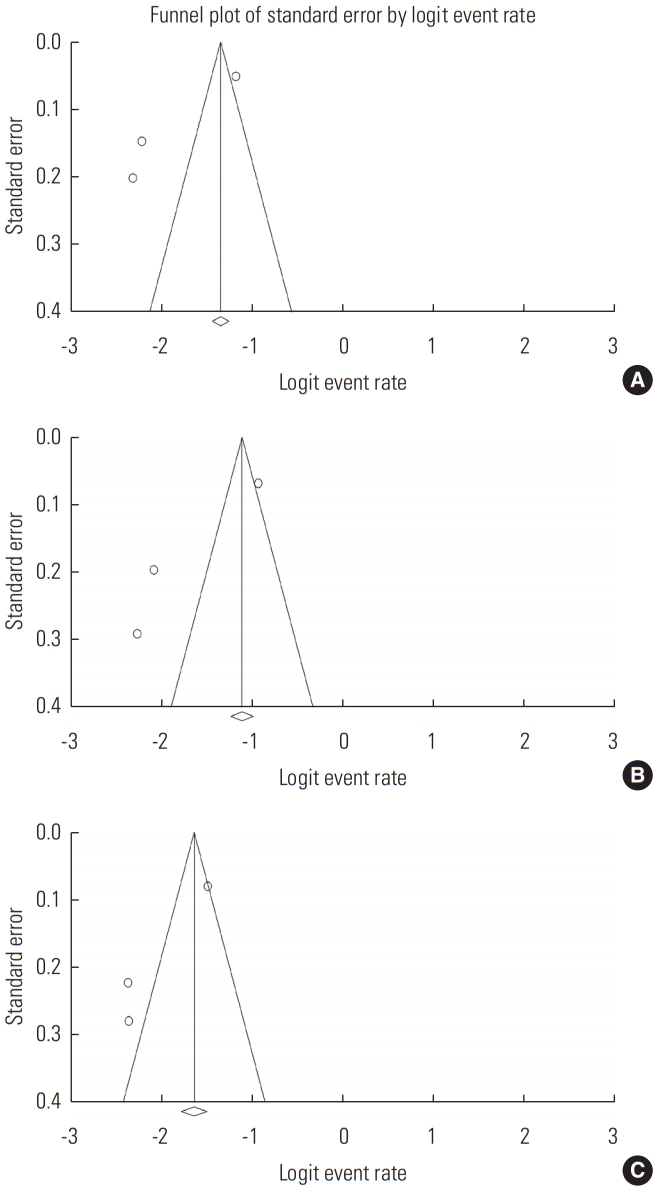
- Publication Bias
- Funnel plot analysis and the Egger test were performed. Funnel-plot analyses revealed symmetrical results (Figure 3). In addition, all p-values for the Egger test were >0.05 (total prevalence among elderly people: p=0.301; prevalence among elderly men: p=0.069; prevalence among elderly women: p=0.059). Therefore, publication bias was not significant.
RESULTS
- A meta-analysis was performed to determine the prevalence of sarcopenia in the elderly Korean population. The results showed that the overall prevalence was 13.1%; the prevalence in men was 14.9% and that in women was 11.4%. All 3 included studies used the EWGSOP criteria for the diagnosis of sarcopenia.
- Although the results of previous studies on the prevalence of sarcopenia are heterogeneous, generally it has been reported to range from 10% to 20% [14-17]. Our results are similar to those of previous studies. In addition, in our study, men showed a higher prevalence of sarcopenia than women, which is consistent with the results of several previous studies [2,18- 20]. Some possible reasons for this have been suggested. First, the prevalence of sarcopenia increases in patients with diabetes, and since men generally have a higher prevalence of diabetes than women, the prevalence of sarcopenia in men may therefore be higher [21]. Second, a higher prevalence of sarcopenia in men could be related to their higher smoking rate, especially in men in Korea [5,22]. Since smoking decreases the amount of blood flow, the amount of oxygen provided to the muscles is reduced. In addition, smoking interferes with normal breathing, and consequently, gas exchange in the lungs cannot be performed normally, which makes it difficult for the muscles to receive oxygen [23]. When muscles are not properly supplied with oxygen, muscle growth is inhibited, which causes sarcopenia. Third, higher alcohol consumption in Korean men could result in a higher prevalence of sarcopenia in men [14,24]. It has been reported that alcohol reduces the synthesis of proteins [25]. Since protein synthesis in muscles is an essential factor for muscle growth, excessive alcohol consumption increases the probability of developing sarcopenia [26]. Thus, stopping or reducing smoking and alcohol consumption in the elderly population would be helpful for preventing and treating sarcopenia. Furthermore, at least 2-4 sessions of combined aerobic exercise and resistance training every week and appropriate protein intake (at least 1 g/kg) are essential for the prevention and treatment of sarcopenia [27].
- Regarding the prevalence of sarcopenia in other countries, Du et al. [28] surveyed 2458 elderly individuals (≥65 years of age) in the United States and reported that the total prevalence of sarcopenia was 15.51%. Lera et al. [29] reported that the prevalence of sarcopenia in 1006 elderly individuals (≥60 years of age) in Santiago, Chile was 19.1%. Liu et al. [30] investigated the prevalence of sarcopenia in 4500 elderly individuals (>60 years of age) in Yunnan, Guizhou, Sichuan, and Xinjiang in China and found it to be 19.3%. Generally, the prevalence of sarcopenia in Korea is lower than that in other countries. A variety of factors, such as differences in eating habits, the surrounding environment, culture, and race-specific genetics, may be responsible for differences in the prevalence of sarcopenia among countries [31-33].
- To date, over a dozen studies have attempted to examine the prevalence of sarcopenia in Korea. However, the 3 studies included in our meta-analysis were the only ones that measured muscle function for the diagnosis of sarcopenia, instead of only considering appendicular muscle mass. Sarcopenia is defined as a condition characterized by loss of both skeletal muscle mass and function. Muscle strength depends on muscle mass, and the relationship between muscle strength and muscle mass is not linear [13]. Therefore, for the diagnosis of sarcopenia, both muscle mass and muscle function must be measured.
DISCUSSION
- We found that the overall prevalence of sarcopenia in the elderly Korean population was 13.1%. The prevalence of sarcopenia in elderly men and women was 14.9% and 11.4%, respectively. This is the first study to systematically evaluate the prevalence of sarcopenia in Korea through a meta-analysis. However, our study is limited by the inclusion of a small number of studies and population. For more robust results, further well-designed studies with larger populations should be conducted in the future.
CONCLUSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
The present study was supported by a National Research Foundation of Korea grant funded by the Korean government (grant No. NRF-2019M3E5D1A02068106).
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Conceptualization: YJC, MCC. Data curation: YJC, MCC. Formal analysis: YJC, MCC. Funding acquisition: MCC. Methodology: YJC, MCC. Visualization: YJC, MCC. Writing – original draft: YJC, MCC. Writing – review & editing: YJC, MCC.
Notes


| Study | Study design | Subjects (n, age, M:F) | Definition of sarcopenia | Body composition assessment | Muscle function assessment | Participant recruitment method | Region |
|---|---|---|---|---|---|---|---|
| Jung et al., 2019 [10] | Cross-sectional | 521, 71.6 y, 263:258 | EWGSOP | BIA | Handgrip strength | National Fitness Award Project in 2014-2015 | Nationwide |
| Kim et al., 2016 [11] | Cross-sectional | 302, 75.0 y, 139:163 | EWGSOP | DXA | Handgrip strength, 6-meter usual gait speed | Hallym Aging Study data in 2010 | Chuncheon |
| Kim et al., 2019 [12] | Cross-sectional | 2099, 75.9 y, 1053:1046 | EWGSOP | DXA, BIA | Handgrip strength, chair stand test (five times sit-to-stand test) | The nationwide Korean Frailty and Aging Cohort Study in 2016-2017 | Nationwide |
- 1. Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol 2012;24(6):623-627ArticlePubMedPMC
- 2. Tay L, Ding YY, Leung BP, Ismail NH, Yeo A, Yew S, et al. Sex-specific differences in risk factors for sarcopenia amongst community-dwelling older adults. Age (Dordr) 2015;37(6):121ArticlePubMedPMC
- 3. Silva RF, Figueiredo MD, Darder JJ, Santos AM, Tyrrell MA. Sarcopenia screening in elderly in primary health care: nurse knowledge and practices. Rev Bras Enferm 2020;73(Suppl 3):e20200421ArticlePubMed
- 4. Jang HC. How to diagnose sarcopenia in Korean older adults? Ann Geriatr Med Res 2018;22(2):73-79ArticlePubMedPMC
- 5. Kim YS, Lee Y, Chung YS, Lee DJ, Joo NS, Hong D, et al. Prevalence of sarcopenia and sarcopenic obesity in the Korean population based on the Fourth Korean National Health and Nutritional Examination Surveys. J Gerontol A Biol Sci Med Sci 2012;67(10):1107-1113ArticlePubMed
- 6. Moon JH, Kong MH, Kim HJ. Implication of sarcopenia and sarcopenic obesity on lung function in healthy elderly: using Korean National Health and Nutrition Examination Survey. J Korean Med Sci 2015;30(11):1682-1688ArticlePubMedPMC
- 7. Woo N, Kim SH. Sarcopenia influences fall-related injuries in community-dwelling older adults. Geriatr Nurs 2014;35(4):279-282ArticlePubMed
- 8. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6(7):e1000097ArticlePubMedPMC
- 9. Luchini C, Stubbs B, Solmi M, Veronese N. Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World J Metaanal 2017;5(4):80-84Article
- 10. Jung M, Park S, Kim H, Kwon O. Association of diet quality with low muscle mass-function in Korean elderly. Int J Environ Res Public Health 2019;16(15):2733ArticlePubMedPMC
- 11. Kim JH, Kim DH, Park YS. Body composition, sarcopenia, and suicidal ideation in elderly Koreans: Hallym Aging Study. J Korean Med Sci 2016;31(4):604-610ArticlePubMedPMC
- 12. Kim M, Won CW. Prevalence of sarcopenia in community-dwelling older adults using the definition of the European Working Group on Sarcopenia in Older People 2: findings from the Korean Frailty and Aging Cohort Study. Age Ageing 2019;48(6):910-916ArticlePubMed
- 13. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010;39(4):412-423ArticlePubMedPMC
- 14. Sun S, Lee H, Yim HW, Won HS, Ko YH. The impact of sarcopenia on health-related quality of life in elderly people: Korean National Health and Nutrition Examination Survey. Korean J Intern Med 2019;34(4):877-884ArticlePubMed
- 15. Kim SH, Kwon HS, Hwang HJ. White blood cell counts, insulin resistance, vitamin D levels and sarcopenia in Korean elderly men. Scand J Clin Lab Invest 2017;77(3):228-233ArticlePubMed
- 16. Kim TN, Lee EJ, Hong JW, Kim JM, Won JC, Kim MK, et al. Relationship between sarcopenia and albuminuria: the 2011 Korea National Health and Nutrition Examination Survey. Medicine (Baltimore) 2016;95(3):e2500PubMedPMC
- 17. Yoo JI, Choi H, Ha YC. Mean hand grip strength and cut-off value for sarcopenia in Korean adults using KNHANES VI. J Korean Med Sci 2017;32(5):868-872ArticlePubMedPMC
- 18. Brown JC, Harhay MO, Harhay MN. Sarcopenia and mortality among a population-based sample of community-dwelling older adults. J Cachexia Sarcopenia Muscle 2016;7(3):290-298ArticlePubMed
- 19. Chan R, Leung J, Woo J. A prospective cohort study to examine the association between dietary patterns and sarcopenia in Chinese community-dwelling older people in Hong Kong. J Am Med Dir Assoc 2016;17(4):336-342ArticlePubMed
- 20. Spira D, Norman K, Nikolov J, Demuth I, Steinhagen-Thiessen E, Eckardt R. Prevalence and definition of sarcopenia in community dwelling older people. Data from the Berlin aging study II (BASE-II). Z Gerontol Geriatr 2016;49(2):94-99ArticlePubMed
- 21. Wang T, Feng X, Zhou J, Gong H, Xia S, Wei Q, et al. Type 2 diabetes mellitus is associated with increased risks of sarcopenia and pre-sarcopenia in Chinese elderly. Sci Rep 2016;6: 38937ArticlePubMedPMC
- 22. Kim JE, Lee YH, Huh JH, Kang DR, Rhee Y, Lim SK. Early-stage chronic kidney disease, insulin resistance, and osteoporosis as risk factors of sarcopenia in aged population: the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV), 2008-2009. Osteoporos Int 2014;25(9):2189-2198ArticlePubMed
- 23. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: Implications for electronic cigarette use. Trends Cardiovasc Med 2016;26(6):515-523ArticlePubMedPMC
- 24. Kim CR, Jeon YJ, Jeong T. Risk factors associated with low handgrip strength in the older Korean population. PLoS One 2019;14(3):e0214612ArticlePubMedPMC
- 25. Rom O, Kaisari S, Aizenbud D, Reznick AZ. Lifestyle and sarcopenia—etiology, prevention, and treatment. Rambam Maimonides Med J 2012;3(4):e0024ArticlePubMedPMC
- 26. Lieber CS. Relationships between nutrition, alcohol use, and liver disease. Alcohol Res Health 2003;27(3):220-231PubMedPMC
- 27. Marcell TJ. Sarcopenia: causes, consequences, and preventions. J Gerontol A Biol Sci Med Sci 2003;58(10):M911-M916PubMed
- 28. Du K, Goates S, Arensberg MB, Pereira S, Gaillard T. Prevalence of sarcopenia and sarcopenic obesity vary with race/ethnicity and advancing age. Divers Equal Health Care 2018;15(4):175-183Article
- 29. Lera L, Albala C, Sánchez H, Angel B, Hormazabal MJ, Márquez C, et al. Prevalence of sarcopenia in community-dwelling Chilean elders according to an adapted version of the European Working Group on Sarcopenia in Older People (EWGSOP) criteria. J Frailty Aging 2017;6(1):12-17PubMed
- 30. Liu X, Hao Q, Yue J, Hou L, Xia X, Zhao W, et al. Sarcopenia, obesity and sarcopenia obesity in comparison: prevalence, metabolic profile, and key differences: results from WCHAT study. J Nutr Health Aging 2020;24(4):429-437ArticlePubMed
- 31. Barbieri E, Agostini D, Polidori E, Potenza L, Guescini M, Lucertini F, et al. The pleiotropic effect of physical exercise on mitochondrial dynamics in aging skeletal muscle. Oxid Med Cell Longev 2015;2015: 917085ArticlePubMedPMC
- 32. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health 2018;6(10):e1077-e1086ArticlePubMed
- 33. Lee JE, McLerran DF, Rolland B, Chen Y, Grant EJ, Vedanthan R, et al. Meat intake and cause-specific mortality: a pooled analysis of Asian prospective cohort studies. Am J Clin Nutr 2013;98(4):1032-1041ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Phenotype validation of the Korean working group on sarcopenia guideline
Sunghwan Ji, Ji Yeon Baek, Eunju Lee, Il-Young Jang, Hee-Won Jung
Archives of Gerontology and Geriatrics.2024; 117: 105251. CrossRef - The prevalence and factors associated with sarcopenia in Thai older adults: A systematic review and meta-analysis
Phatcharaphon Whaikid, Noppawan Piaseu
International Journal of Nursing Sciences.2024; 11(1): 31. CrossRef - Association of low muscle mass and obesity with increased all‐cause and cardiovascular disease mortality in US adults
Donghyun Kim, Junghoon Lee, Raekil Park, Chang‐Myung Oh, Shinje Moon
Journal of Cachexia, Sarcopenia and Muscle.2024; 15(1): 240. CrossRef - Sonographic methods to predict type 2 diabetes patients with sarcopenia: B mode ultrasound and shear wave elastography
Shengqiao Wang, Xinliang Xu, Siqi Cao, Juan Cheng, Ying Wang, Yi Dong
Clinical Hemorheology and Microcirculation.2024; : 1. CrossRef - Relationship between asthma and sarcopenia in the elderly: a nationwide study from the KNHANES
Ha-Kyeong Won, Yewon Kang, Jin An, Ji-Hyang Lee, Woo-Jung Song, Hyouk-Soo Kwon, You Sook Cho, Hee-Bom Moon, Il-Young Jang, Tae-Bum Kim
Journal of Asthma.2023; 60(2): 304. CrossRef - Correlation between temporal muscle thickness and grip strength in hemiplegic patients with acute stroke
Jisoo Park, Jihye Park, Soye Kim, Dong Chan Kim
Frontiers in Neurology.2023;[Epub] CrossRef - Impact of sarcopenia and phase angle on mortality of the very elderly
Young Eun Kwon, Jung Sun Lee, Jee‐young Kim, Song In Baeg, Hye Min Choi, Hong‐Bae Kim, Joon Young Yang, Dong‐Jin Oh
Journal of Cachexia, Sarcopenia and Muscle.2023; 14(1): 279. CrossRef - The effect of combining nutrient intake and physical activity levels on central obesity, sarcopenia, and sarcopenic obesity: a population-based cross-sectional study in South Korea
Jong Eun Park, Seulgi Lee, Kirang Kim
BMC Geriatrics.2023;[Epub] CrossRef - Prevalence of sarcopenia in patients with COPD through different musculature measurements: An updated meta-analysis and meta-regression
Jie He, Hezhi Li, Jun Yao, Yan Wang
Frontiers in Nutrition.2023;[Epub] CrossRef - Association between Sarcopenia, Falls, and Cognitive Impairment in Older People: A Systematic Review with Meta-Analysis
Jack Roberto Silva Fhon, Alice Regina Felipe Silva, Eveline Fontes Costa Lima, Alexandre Pereira dos Santos Neto, Ángela Maria Henao-Castaño, Elizabeth Fajardo-Ramos, Vilanice Alves Araújo Püschel
International Journal of Environmental Research and Public Health.2023; 20(5): 4156. CrossRef - COVID-19 in Older Patients: Assessment of Post-COVID-19 Sarcopenia
Almudena López-Sampalo, Lidia Cobos-Palacios, Alberto Vilches-Pérez, Jaime Sanz-Cánovas, Antonio Vargas-Candela, Juan José Mancebo-Sevilla, Halbert Hernández-Negrín, Ricardo Gómez-Huelgas, María Rosa Bernal-López
Biomedicines.2023; 11(3): 733. CrossRef - The High Prevalence of Sarcopenia in Rheumatoid Arthritis in the Korean Population: A Nationwide Cross-Sectional Study
Dongwoo Kim, Yu Jin Lee, Eui Seop Song, Ahreum Kim, Cho Hee Bang, Jae Hyun Jung
Healthcare.2023; 11(10): 1401. CrossRef - Lack of association between serum myonectin levels and sarcopenia in older Asian adults
Sunghwan Ji, So Jeong Park, Jin Young Lee, Ji Yeon Baek, Hee-Won Jung, Kyunggon Kim, Hyun Ju Yoo, Il-Young Jang, Beom-Jun Kim
Experimental Gerontology.2023; 178: 112229. CrossRef - Research Progress of Sarcopenia
苗 段
Advances in Clinical Medicine.2023; 13(05): 8836. CrossRef - Prevalence of Sarcopenia in Africa: A Systematic Review
Bryan Vincent Mballa Yene, Sang-Yeob Lee, Ki-Soo Park, Yang Jae Kang, Sung Hyo Seo, Jun-Il Yoo
Clinical Interventions in Aging.2023; Volume 18: 1021. CrossRef - Efficacy of Silkworm Pupae Extract on Muscle Strength and Mass in Middle-Aged and Older Individuals: A Randomized, Double-Blind, Placebo-Controlled Trial
J.I. Choi, H.Y. Kweon, Y.L. Lee, J.H. Lee, Sang Yeoup Lee
The Journal of nutrition, health and aging.2023; 27(7): 578. CrossRef - The Impact of Possible Sarcopenia and Obesity on the Risk of Falls in Hospitalized Older Patients
Kahyun Kim, Dukyoo Jung
The Korean Journal of Rehabilitation Nursing.2023; 26(1): 18. CrossRef - Editorial: (Osteo)sarcopenia & sarcopenic obesity, volume II
Ifigenia Kostoglou-Athanassiou, Lambros Athanassiou, Panagiotis Athanassiou, Stefano Masiero, Yannis Dionyssiotis
Frontiers in Endocrinology.2023;[Epub] CrossRef - Highlighting Unseen Activity: A 48-Hour Continuous Measurement in Subacute Stroke Rehabilitation – A Preliminary Cohort Study (Preprint)
Emi Mizuno, Masahiko Mukaino, Takayuki Ogasawara, Masumi Yamaguchi, Shingo Tsukada, Shigeru Sonoda, Yohei Otaka
JMIR Formative Research.2023;[Epub] CrossRef - Research Progress on Pathogenesis and Drug Treatment of Hypertension Complicated with Sarcopenia
晓琼 张
Advances in Clinical Medicine.2022; 12(05): 4132. CrossRef - Impact of Sarcopenia and Bone Mineral Density on Implant Failure after Dorsal Instrumentation in Patients with Osteoporotic Vertebral Fractures
Harald Krenzlin, Leon Schmidt, Dragan Jankovic, Carina Schulze, Marc A. Brockmann, Florian Ringel, Naureen Keric
Medicina.2022; 58(6): 748. CrossRef - An analysis study of sarcopenia and locomotive syndrome in the old people using evaluation tool
Myung-Chul Kim, Hang-Sik Park, Hae-In Kim, Jean-Kyung Park, Dong-Kun Chung
Journal of Exercise Rehabilitation.2022; 18(4): 256. CrossRef - The Positive Association between Muscle Mass and Bone Status Is Conserved in Men with Diabetes: A Retrospective Cross-Sectional and Longitudinal Study
Hyun Uk Moon, Seung Jin Han, Hae Jin Kim, Yoon-Sok Chung, Dae Jung Kim, Yong Jun Choi
Journal of Clinical Medicine.2022; 11(18): 5370. CrossRef - Prevalence of sarcopenia in Chinese community-dwelling elderly: a systematic review
Xiaoyu Ren, Xianliang Zhang, Qiang He, Litao Du, Ke Chen, Si Chen, Yang Pan
BMC Public Health.2022;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite