
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 55(6); 2022 > Article
-
Original Article
Intervention to Improve Menstrual Health Among Adolescent Girls Based on the Theory of Planned Behavior in Iran: A Cluster-randomized Controlled Trial -
Fatemeh Darabi1
 , Mehdi Yaseri2
, Mehdi Yaseri2 -
Journal of Preventive Medicine and Public Health 2022;55(6):595-603.
DOI: https://doi.org/10.3961/jpmph.22.365
Published online: November 30, 2022
- 2,433 Views
- 102 Download
- 2 Scopus
1Department of Public Health, Asadabad School of Medical Sciences, Asadabad, Iran
2Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
- Corresponding author: Mehdi Yaseri, Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran 141556446, Iran E-mail: m.yaseri@gmail.com
Copyright © 2022 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives:
- Poor menstrual health may lead to school absenteeism and adverse health outcomes for adolescents. The purpose of this study was to determine the effect of pubertal and menstrual health education on health and preventive behaviors among Iranian secondary school girls.
-
Methods:
- A quasi-experimental study was conducted to evaluate the effectiveness of a health intervention program. A total of 578 students (including intervention and control participants) in 12 schools in Tehran Province, Iran were included by multistage random sampling. The program comprised seven 2-hour educational sessions. After confirming the reliability and validity of a researcher-made questionnaire, that questionnaire was used to collect the required data, and the groups were followed up with after 6 months.
-
Results:
- After the educational intervention, the mean scores of menstrual health-related knowledge and constructs of the theory of planned behavior were significantly higher in the intervention group than in the control group (p<0.001 for all dimensions).
-
Conclusions:
- The results of this study emphasize the effectiveness of menstrual health interventions in schools. These findings should also encourage health policy-makers to take committed action to improve performance in schools.
- Adolescence is a stage in which individuals reach sexual maturity [1] and undergo major changes in various aspects of development, including physical, social, and emotional development [2]. Puberty is a transitional period between childhood and adulthood, a stage of rapid growth in which remarkable physical, psychological, and social changes occur [3]. Menstruation is a sign of puberty in adolescent girls [4]. The onset of menstruation should not be seen as a disease or abnormality, but rather as a sign of puberty and fertility. Adolescent girls often do not receive accurate information on menstruation for specific cultural reasons, leading to unhealthy behaviors [2].
- Within the broader areas of education and development, puberty care has been a concern for Iran’s Ministry of Health in recent years. As such, puberty health education is being implemented in some schools in Tehran Province, targeting not only students but also parents and school staff [5]. Many studies on menstrual health issues from around the world have demonstrated the effectiveness of educational interventions among middle and high school girls [6-8]. One study conducted in Nepal revealed that knowledge and practices related to menstruation and puberty were not satisfactory, and those researchers emphasized that health education given by parents, teachers and the mass media is important in dispelling misconceptions about menstrual health [9]. Studies have shown that the pubertal and menstrual health of Iranian girls is poor to moderate [2,4,10].
- One priority of the Ministry of Health and the Ministry of Education is to revise the health education system to improve reproductive health. According to studies on adolescent health, disproportionately little attention has been paid to the needs of this age group [11]. Adolescent girls also do not receive adequate information about menstrual health due to special cultural restrictions [12]. Various studies from around the world have focused on menstrual health issues. Educational interventions among primary and secondary school girls have been shown to be effective [13,14]. Based on the results of related studies, the menstrual health of adolescent girls in Iran over the past decade has been poor [4,15].
- Moreover, inadequate information about bodily changes and a lack of body confidence have been observed in adolescent students, and many have expressed a demand for menstrual health education [16]. Similar studies have reported the existence of little information on menstrual health and menstruation among the majority of adolescent girls [16,17], with most girls viewing menstruation simply as the ability to give birth and perceiving bathing as difficult during menstruation. They also reported considering it inappropriate for girls to talk about their bodies [18]. Further, restrictive rules exist for menstruating females in many cultures and countries [19]. Consequently, adolescent girls encounter multiple problems throughout the reproductive lifespan, particularly once they become pregnant or during menstruation [20]. Generally, girls prefer to acquire information about menstrual health from a range of sources, including parents, friends, and media. Although many sources are available, adolescent girls have expressed a lack of adequate knowledge regarding menstrual health [21].
- The effectiveness of the theory of planned behavior (TPB) in improving healthy behaviors has been previously emphasized [22]. According to the TPB, attitude, subjective norms, and perceived behavioral control are the principal determinants of motivation, which is assessed as the intention to perform a task or behavior, like learning about menstrual health [23]. In this study, we investigated the role of student perception of parental control using the TPB [24]. As such, we added the construct of perceived parental control to the original TPB. To date, few empirical studies have assessed the direct TPB measures (attitudes, subjective norms, and perceived behavioral control) to predict adolescents’ behavior related to menstrual health promotion [24].
- Given the insufficient and inaccurate knowledge and practices regarding menstrual health and menstruation among adolescent girls [3,25], the importance of healthy practices during menstruation [26], and the limited number of theory-based studies on menstrual health education, the present study was conducted to investigate the potential of education to improve pubertal and menstrual health among secondary school girls in Tehran.
INTRODUCTION
- Study Design and Sample Size
- This study incorporated a cluster-randomized controlled trial design. In this study, 578 students were included, with 289 students randomly assigned to the intervention group and 289 students to the control group. Three of the 22 districts in Tehran were initially selected using proportional stratified random sampling. In each selected district, 2 schools were randomly assigned to the control group and 2 schools to the experimental group. Based on random selection, we enrolled 4 schools in each district (12 schools in total), 3 classes in each school (36 classes in total), and 16 students per class (578 students in total). Verbal consent was obtained from all participants and their parents after the purpose and nature of the study were explained. Moreover, participants were assured that their responses and personal information would remain confidential.
- Intervention Program
- The education program was a school-based approach composed of seven 2-hour educational sessions. Topics included the importance of adolescence; the importance of puberty health; improving awareness of menstrual health; physical changes during adolescence; maturity and menstrual health; health habits including bathing the genitals, changing underwear daily to prevent uterine infection, and proper cleaning (first of the vulval and then the anal area) after each defecation; ways to prevent or reduce premenstrual symptoms (headache, pain in the abdomen and/or side, anger, etc.); avoiding going to the swimming pool during this period; paying attention to menstruation patterns, particularly sudden changes; changing the diet, including consuming more protein and less salt and sugar, reducing the consumption of fast food and increasing that of vegetables and fruits, and avoiding certain foods; the ability to engage in social activities; the adverse impact of menstruation on daily activities; handling mood swings such as sadness, depression, and anxiety during menstruation; willingness to be flexible and ability to communicate effectively with others [11]; promotion of student beliefs and attitudes about pubertal and menstrual health; parental support of their children on issues related to pubertal and menstrual health; hygiene during puberty; ability and control of behavior related to menstrual health; and menstrual health promotion skills (Table 1) [11].
- Students in both groups filled out the questionnaire. The educational program lasted for 3 months, and 6 months after the end of the training sessions, the students were asked to complete the questionnaire again. The control group comprised high school students in Tehran Province who did not participate in the educational intervention.
- In this study, a questionnaire developed by the researcher was used for data collection before and after the educational intervention [27,28]. This questionnaire comprised 42 items in 3 parts.
- The first part contained participants’ demographic information, including age, father’s employment, mother’s employment, father’s education, mother’s education, and economic status.
- The second part of the questionnaire included questions about menstrual and pubertal health awareness. A set of 10 questions with 3 response levels (true, false, and unknown) was used.
- The third section concerned the TPB constructs and included 11 questions about the individual’s menstrual and pubertal health attitudes, 7 questions about subjective norms, 6 questions about behavioral intentions, 6 questions about perceived behavioral control, 4 questions about perceived parental control, and 8 questions about behavior.
- The score for each item ranged from 1 (strongly disagree) to 5 (strongly agree) based on a 5-point Likert-style scale. In addition, the total score was converted to a 100-point scale. This questionnaire was developed based on direct TPB measures regarding various issues associated with menstrual health.
- Validity and Reliability
- We determined the validity and reliability of the questionnaire. The validity of the questionnaire was assessed in terms of face and content validity, which were determined based on the viewpoints of the adolescent girls, health sciences specialists, and experts in the community. The reliability of the scale was assessed based on the internal consistency and stability of the scale. The test-retest scores for every construct were compared using Pearson correlations. An internal correlation coefficient greater than 0.40 was considered acceptable [29]. The results of the test-retest reliability analysis over a 2-week period indicated that the questionnaire was stable (internal correlation coefficient, 0.82). The internal consistency was assessed using the Cronbach’s α value to determine the scale’s reliability. The Cronbach’s α coefficient revealed an excellent internal consistency (α=0.92 overall, ranging from 0.96 to 0.97 for different TPB constructs).
- Statistical Analysis
- The data were entered into SPSS version 23 (IBM Corp., Armonk, NY, USA) after collection, processing, and organization. To facilitate comparison of our results with those of other studies, we converted the scores of the TPB constructs into a 100- point scale. A multilevel approach was used to investigate the associations of the measurements in 2 groups. In addition, the likelihood ratio test was used to find the adequate number of levels for the multilevel analysis. Two-level multilevel analysis was used to compare baseline measures between the groups. Three-level multilevel analysis was used to assess the changes in each group. In addition, we included the interactions between groups and time in the multilevel analysis. Thus, we could compare the changes in the scores of the TPB constructs and conduct an intention-to-treat analysis. A p-value of less than 0.05 was considered to indicate statistical significance.
- Ethics Statement
- Ethical approval was obtained from the Ethics Committee of Tehran University of Medical Sciences (IR.TUMS.REC.1394.651 and code IRCT2015070623089N2) for this research project.
METHODS
- In this study, the average age of the adolescents was 14.1±1.0 years. The socioeconomic level was categorized as very good for 6.1%, good for 41.9%, average for 43.9%, and poor for 8.1% of the participants. Among the study participants, almost two-thirds of both fathers (63.8%) and mothers (65.8%) had between 6 years and 12 years of education. Regarding parental employment status, 94.1% of fathers were employed and 5.9% were unemployed, while of the mothers, 26.5% were employed and 73.5% were housewives (Table 2). No significant difference was found between the 2 groups in terms of demographic variables (age, parents’ education, parents’ employment, and financial condition) before the educational intervention (Table 2).
- As shown in Table 3, no significant difference was found between groups in the mean scores of menstrual health knowledge and of the TPB constructs before the intervention. Significant interaction effects between the groups and time were found for the TPB constructs and knowledge after the intervention program (p<0.001). After the intervention, the knowledge score significantly increased in the intervention group (p<0.001).
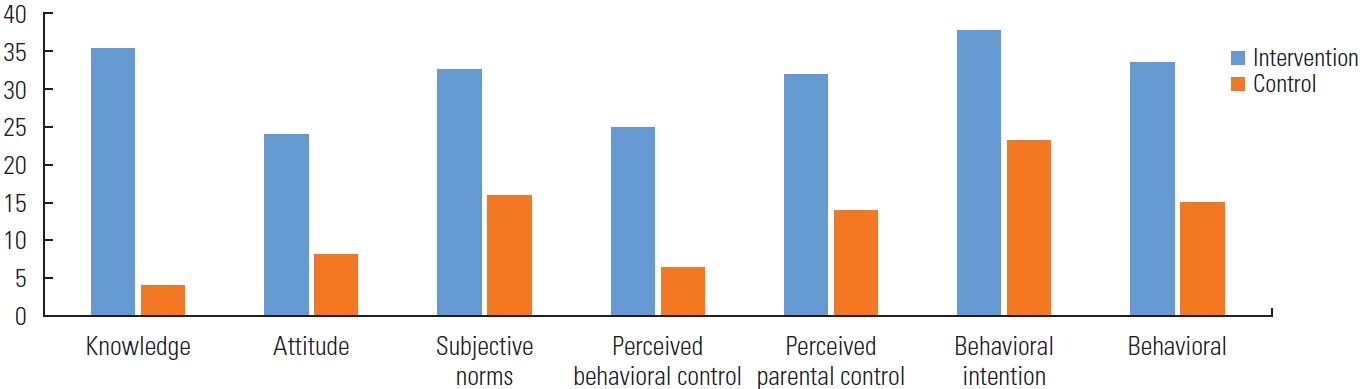
- Among the most noteworthy results was the impact of the educational intervention on menstrual health knowledge. In the intervention group, the mean score for knowledge increased from 49.1 before the intervention to 84.3 at the 6-month follow-up, constituting a significant difference (p<0.001). The mean score for menstrual attitude increased from 68.6 to 92.6 in the intervention group over the same period (p<0.001). Additionally, in the intervention group, the mean score of subjective norms increased from 61.7 to 94.2 (p<0.001), the mean score of behavioral intention increased from 69.3 to 94.2 (p<0.001), and the mean score of perceived behavioral control increased from 63.0 to 94.9 (p<0.001). The mean score of perceived parental support regarding necessary training and guidance about menstruation and puberty-related issues increased from 57.1 to 94.6 in the intervention group (p<0.001). Finally, the mean score for behavior increased from 60.8 to 94.3 in the intervention group (p<0.001) (Figure 1 and Table 3).
RESULTS
- According to these results, TPB-based education programs are effective in modifying psychosocial aspects related to menstrual health among adolescents. Such programs could also have benefits in fields such as health, education, and development.
- And this sentence should be deleted: The present study results indicate a significant difference in menstrual health between the intervention and control groups, providing support for participation in adolescent health care programs.
- The results of the baseline survey demonstrated inadequate knowledge about menstrual health among the female adolescent participants, which is an important risk factor for certain reproductive infections. Thus, establishment of a health program for adolescent girls during puberty is essential [30]. Programs can involve parents, mass media, and health care professionals in schools, all playing an important role in the transmission of awareness related to puberty and menstrual health. Therefore, we can conclude that menstrual health education can demonstrably improve the knowledge of adolescent girls about menstrual health. Singh et al. [31] conducted a similar study on the importance of school-based menstrual health education of students and their parents for increasing menstrual health among students. A study in Iran [4] showed the effectiveness of a menstrual health intervention program in high schools, and the authors recommended expanding this program to more schools. These results highlight the pressing need for comprehensive menstrual health education for adolescents, particularly in a country like Iran with a relatively high population of teens and young people [32] where no formal education about menstrual health exists in the school system. A high-quality menstrual health education program coupled with behavior modification may diminish the unpleasant experience of menstruation.
- The present study results indicated a statistically significant difference in the attitude scores of the intervention group (p<0.001) between baseline and after the intervention. Promoting a positive attitude is an approach used in such educational interventions to motivate behavior. Therefore, the positive attitudes of girls toward menstruation are also closely related to puberty health. Thus, fostering accurate and positive beliefs about puberty and menstrual health (such as consuming safe foods; controlling mood swings such as sadness, depression, and anxiety during puberty; embracing flexibility and the ability to communicate effectively with others; changing underwear daily to prevent uterine infection; and personal hygiene during menstruation [such as cleaning the vulval and anal areas after each excretion and defecation]) decreases the absence of female students in schools due to menstrual health-related problems, thereby showing the positive effects of promoting menstrual health in girls. This aligns with the findings of Dipti and Chandra [33]. Research conducted in Iran also aligns with the present study in the consideration of menstrual health as an important part of a female student’s family-related and overall health [4]. Group discussions and workshops may also be implemented to promote a positive attitude toward menstrual health issues. Nevertheless, appropriate educational techniques should be employed to improve adolescent girls’ attitudes toward menstrual health issues. Various studies have shown that health education increases positive attitudes toward puberty and facilitates the acceptance of pubescent changes as a natural physiological phenomenon [4].
- Subjective norms are intended to measure the perceived expectations of others that affect a person’s behaviors. A significant increase in the score of subjective norms was observed in both groups after the intervention (p<0.001). This could support the assumption that the presence of family and other close individuals increased the students’ scores of subjective norms associated with menstrual health. In this study’, subjective norms were investigated from the viewpoints of parents, teachers, advisors, friends, and classmates. Examples included the participant’s perception of family members and others around her believing that she engages in social activities during her menstrual period similar to other times, that she consumes a proper diet during the period of menstruation, and that she looks after her personal menstrual health (bathing, changing underwear, etc.) to prevent any infection. Other items related to whether friends and classmates would agree that the participant lacks the desire to do homework due to changes in mood and depression caused by menstruation, as well as to their encouragement regarding engaging in social activities, such as attending social meetings, during puberty. Naturally, peer pressure is far greater among students who spend more time engaged in social activity outside of the home. Several studies [34,35] have been conducted to improve subjective norms regarding behavior through TPB constructs. Consequently, attention should be paid to subjective norms as an influential factor in health behavior change.
- A statistically significant difference was also found between the intervention and control groups in perceived behavioral control around menstrual health, providing support for the enrollment of adolescent students in care programs (p<0.001). Poor self-efficacy and personal control regarding behaviors associated with menstrual health is a risk factor for puberty-related and reproductive problems [14]. Thus, perceived behavioral control plays an important role in the promotion of menstrual health care in girls. Examples include handling mood swings such as sadness, depression, and anxiety during menstruation; engaging in healthy practices during the menstrual period (such as bathing, changing underwear, etc.); and choosing to engage in social activities during the menstrual period as during ordinary days. Kaveh et al. [23] conducted a similar study of secondary school girls that showed that educational programs in schools for girls and their parents are effective and play an important role in improving health care. This aligns with the results obtained by Khalajabadi Farahani et al. [14]. According to the concept of perceived behavioral control, people’s behavior is guided by their perceptions regarding their abilities to perform the given behavior [36]. Therefore, along with a strong attitude and subjective norms around a behavior, individuals should have voluntary control over their behavior to become capable of performing the behavior in question [36].
- Parents can play a positive and supportive role in promoting girls’ pubertal and menstrual health. In fact, they can impact their children’s menstrual health through care and control. In the present study, after the intervention, the mean score for perceived parental control was significantly higher in the intervention group than in the control group (p<0.001). According to the results of this study and similar studies, parental support can promote the adolescent’s acquisition of adequate information about menstruation health [14]. In a study conducted in Iran, Fakhri et al. [4] emphasized the importance of the parental role in the menstrual health of school girls in the city of Mazandaran.
- Based on the study results, a TPB-based educational intervention improved students’ intentions around performing preventive behaviors and thus improve menstrual health. This finding is consistent with the results of a study by Darabi et al. [37], who investigated the effect of an educational intervention program on female students’ participation in a sexual and reproductive health educational program, with a positive effect on the adolescent girls’ behavior and health promotion. According to the findings of the present study, health education programs in schools can constitute effective intervention to improve pubertal and menstrual health. Similar to the intervention group, the mean scores of knowledge and all TPB constructs slightly increased in the control group, but these increases were not statistically significant. Such increases in the scores of the control group are unsurprising, since some puberty health education has been recently added to the Iranian school curriculum. Furthermore, the baseline questions may have aroused the students’ curiosity about puberty health issues. Other studies have also reported a slight increase in the scores of the control group [38,39]. Nevertheless, the possible role of sample size in determining statistical significance cannot be ignored.
- The results of this trial showed the effectiveness of an educational intervention on pubertal and menstrual health. One beneficial result of this study is that it encourages policy-makers to increase their commitment to improving performance in schools and include more information on puberty and menstruation in curricula. Officials should also consider campaigns in the community to reduce social taboos about menstruation. Therefore, we suggest that TPB structures should be used in the design and implementation of educational intervention programs, including those regarding health behaviors for adolescent girls [11].
- One of the strengths of the present study is the validation of the TPB-based questionnaire by health education and health promotion specialists and the use of factor analysis for validation. However, the implementation of this study in urban areas and among adolescent girls was a limitation of this study. Therefore, the results can be generalized only to teenage girls in Tehran, and not to other geographical areas.
DISCUSSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
None.
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Both authors contributed equally to conceiving the study, analyzing the data, and writing this paper.
Notes
| Structures | Total | Intervention | Control | Diff |
95% CI |
p-value | ||
|---|---|---|---|---|---|---|---|---|
| LL | UL | |||||||
| Knowledge about menstrual health | Pre | 49.2±20.6 | 49.1±20.6 | 49.3±20.6 | -0.2 | -4.1 | 3.7 | >0.991 |
| Post | 68.7±24.3 | 84.3±13.4 | 53.2±22.8 | 27.0 | 23.8 | 30.2 | <0.0012 | |
| Change | 19.7±28.2 | 35.2±23.9 | 4.1±23.2 | 27.0 | 23.0 | 31.0 | ||
| p-within1 | <0.001 | 0.219 | ||||||
| Students' beliefs and attitudes about puberty and menstrual health | Pre | 68.6±14.3 | 68.6±14.3 | 68.6±14.3 | -0.2 | -1.3 | 0.8 | 0.6981 |
| Post | 84.7±13.3 | 92.6±7.7 | 76.9±13.0 | 17.5 | 15.9 | 19.0 | <0.0012 | |
| Change | 16.1±19.4 | 24.0±16.3 | 8.2±19.1 | 17.7 | 15.9 | 19.4 | ||
| p-within1 | <0.001 | <0.001 | ||||||
| Subjective norms about menstrual health | Pre | 61.7±13.8 | 61.7±13.8 | 61.7±13.8 | 0.2 | -0.7 | 1.1 | 0.6451 |
| Post | 85.9±14.2 | 94.2±8.9 | 77.6±13.8 | 15.9 | 14.3 | 17.6 | <0.0012 | |
| Change | 24.2±20.1 | 32.5±16.6 | 16.0±19.8 | 15.7 | 13.9 | 17.5 | ||
| p-within1 | <0.001 | <0.001 | ||||||
| Behavioral intentions about menstrual health | Pre | 69.4±16.2 | 69.3±16.2 | 69.5±16.2 | -0.2 | -2.3 | 1.9 | 0.8051 |
| Post | 85.0±13.4 | 94.2±7.2 | 75.7±11.7 | 19.9 | 18.3 | 21.4 | <0.0012 | |
| Change | 15.6±21.0 | 24.9±17.4 | 6.3±20.2 | 19.9 | 17.3 | 22.4 | ||
| p-within1 | <0.001 | <0.001 | ||||||
| Perceived behavioral control regarding menstrual health promotion | Pre | 63.0±12.9 | 63.0±12.9 | 64.1±12.9 | 1.1 | -0.8 | 3.0 | 0.2541 |
| Post | 85.9±12.5 | 94.9±5.5 | 76.9±11.0 | 19.1 | 17.5 | 20.6 | <0.0012 | |
| Change | 22.4±18.2 | 31.9±14.3 | 12.8±17.2 | 18.0 | 15.5 | 20.4 | ||
| p-within1 | <0.001 | <0.001 | ||||||
| Perceived parental support regarding menstrual health | Pre | 56.8±14.0 | 57.1±14.2 | 56.5±13.7 | 0.6 | -0.1 | 1.3 | 0.0531 |
| Post | 86.1±15.8 | 94.6±9.8 | 77.6±16.0 | 16.6 | 14.5 | 18.7 | <0.0012 | |
| Change | 29.4±21.0 | 37.6±16.8 | 21.1±22.3 | 14.4 | 11.4 | 17.5 | ||
| p-within1 | <0.001 | <0.001 | ||||||
| Behaviors and skills concerning preventive and menstrual health promotion | Pre | 60.8±17.7 | 60.8±17.6 | 60.9±17.8 | 1.0 | -1.0 | 3.0 | 0.3381 |
| Post | 85.1±16.6 | 94.3±10.5 | 75.9±16.4 | 18.7 | 17.0 | 20.4 | <0.0012 | |
| Change | 24.3±24.3 | 33.5±20.8 | 15.0±24.1 | 17.7 | 15.1 | 20.3 | ||
| p-within1 | <0.001 | <0.001 | ||||||
- 1. Getachew S, Abate L, Asres A, Mandefro A. Knowledge, attitude, and practice toward youth-friendly reproductive health services among Mizan-Tepi university students, South-Western Ethiopia. ScientificWorldJournal 2022;2022: 2312407ArticlePubMedPMCPDF
- 2. Yao J, Ziapour A, Abbas J, Toraji R, NeJhaddadgar N. Assessing puberty-related health needs among 10-15-year-old boys: a cross-sectional study approach. Arch Pediatr 2022;29(4):307-311ArticlePubMed
- 3. Tegegn A, Yazachew M, Gelaw Y. Reproductive health knowledge and attitude among adolescents: a community based study in Jimma Town, Southwest Ethiopia. Ethiop J Health Dev 2008;22(3):143-151
- 4. Fakhri M, Hamzehgardeshi Z, Hajikhani Golchin NA, Komili A. Promoting menstrual health among Persian adolescent girls from low socioeconomic backgrounds: a quasi-experimental study. BMC Public Health 2012;12: 193ArticlePubMedPMCPDF
- 5. Dongre AR, Deshmukh PR, Garg BS. The effect of community-based health education intervention on management of menstrual hygiene among rural Indian adolescent girls. World Health Popul 2007;9(3):48-54Article
- 6. Sourav U, Singh R, Gupta B, Singh A. The effect of community-based health education intervention on management of menstrual hygiene and menstrual disorders among rural Indian women. Indian J Prev Soc Med 2021;52(4):191-196
- 7. Rastogi S, Khanna A, Mathur P. Educational interventions to improve menstrual health: approaches and challenges. Int J Adolesc Med Health 2019;33(5):20190024Article
- 8. Jarrahi R, Golmakani N, Mazloom SR, Forouzanfar H. The effect of menstrual health education adopting the peer education method with the participation of mothers on adolescents’ menstrual health behaviors: a clinical trial. J Midwifery Reprod Health 2021;9(1):2582-2589
- 9. Adhikari P, Kadel B, Dhungel SI, Mandal A. Knowledge and practice regarding menstrual hygiene in rural adolescent girls of Nepal. Kathmandu Univ Med J 2007;5(3):382-386
- 10. Gharacheh M, Ranjbar F, Hajinasab N, Haghani S. Acceptability and safety of the menstrual cups among Iranian women: a cross-sectional study. BMC Womens Health 2021;21(1):105ArticlePubMedPMCPDF
- 11. Valizade R, Taymoori P, Yousefi FY, Rahimi L, Ghaderi N. The effect of puberty health education based on health belief model on health behaviors and preventive among teen boys in Marivan, north west of Iran. Int J Pediatr 2016;4(8):3271-3281
- 12. Golchin NA, Hamzehgardeshi Z, Fakhri M, Hamzehgardeshi L. The experience of puberty in Iranian adolescent girls: a qualitative content analysis. BMC Public Health 2012;12: 698ArticlePubMedPMCPDF
- 13. Dongre AR, Deshmukh PR, Garg BS. A community based approach to improve health care seeking for newborn danger signs in rural Wardha, India. Indian J Pediatr 2009;76(1):45-50ArticlePubMedPDF
- 14. Khalajabadi Farahani F, Darabi F, Yaseri M. The effect of theory-based HIV/AIDS educational program on preventive behaviors among female adolescents in Tehran: a randomized controlled trial. J Reprod Infertil 2020;21(3):194-206PubMedPMC
- 15. Merikangas KR, Nakamura EF, Kessler RC. Epidemiology of mental disorders in children and adolescents. Dialogues Clin Neurosci 2009;11(1):7-20ArticlePubMedPMC
- 16. Ahmmed F, Chowdhury MS, Helal SM. Sexual and reproductive health experiences of adolescent girls and women in marginalised communities in Bangladesh. Cult Health Sex 2022;24(8):1035-1048ArticlePubMed
- 17. Sahiledengle B, Atlaw D, Kumie A, Tekalegn Y, Woldeyohannes D, Agho KE. Menstrual hygiene practice among adolescent girls in Ethiopia: a systematic review and meta-analysis. PLoS One 2022;17(1):e0262295ArticlePubMedPMC
- 18. Chavula MP, Svanemyr J, Zulu JM, Sandøy IF. Experiences of teachers and community health workers implementing sexuality and life skills education in youth clubs in Zambia. Glob Public Health 2022;17(6):926-940ArticlePubMed
- 19. Chabih HD, Elmasry MH. The menstrual taboo and the nuances of misogyny: comparing feminine hygiene TV advertisements in the Arab and western worlds. J Arab Muslim Media Res 2022;15(1):23-44Article
- 20. Latthe P, Latthe M, Say L, Gülmezoglu M, Khan KS. WHO systematic review of prevalence of chronic pelvic pain: a neglected reproductive health morbidity. BMC Public Health 2006;6: 177ArticlePubMedPMCPDF
- 21. Ghandour R, Hammoudeh W, Giacaman R, Holmboe-Ottesen G, Fjeld HE. Coming of age: a qualitative study of adolescent girls’ menstrual preparedness in Palestinian refugee camps in the West Bank and Jordan. Sex Reprod Health Matters 2022;30(1):2111793ArticlePubMedPMC
- 22. Mankarious E, Kothe E. A meta-analysis of the effects of measuring theory of planned behaviour constructs on behaviour within prospective studies. Health Psychol Rev 2015;9(2):190-204ArticlePubMed
- 23. Kaveh MH, Darabi F, Khalajabadi-Farahani F, Yaseri M, Kaveh MH, Mohammadi MJ, et al. The impact of a TPB-based educational intervention on nutritional behaviors in Iranian adolescent girls: a randomized controlled trial. Fresenius Environ Bull 2018;27(6):4349-4356
- 24. De Devitiis B, Viscecchia R, Carfora V, Cavallo C, Cicia G, Del Giudice T, et al. Parents’ trust in food safety and healthiness of children’s diets: a TPB model explaining the role of retailers and government. Econ Agro-Aliment 2021;23(2):1-29
- 25. Kotecha PV, Patel S, Baxi RK, Mazumdar VS, Misra S, Modi E, et al. Reproductive health awareness among rural school going adolescents of Vadodara district. Indian J Sex Transm Dis AIDS 2009;30(2):94-99ArticlePubMedPMC
- 26. Majeed J, Sharma P, Ajmera P, Dalal K. Menstrual hygiene practices and associated factors among Indian adolescent girls: a meta-analysis. Reprod Health 2022;19(1):148ArticlePubMedPMCPDF
- 27. Leung KM, Wong MY, Ou KL, Chung PK, Lau KL. Assessing Esports participation intention: the development and psychometric properties of the theory of planned behavior-based Esports intention questionnaire (TPB-Esport-Q). Int J Environ Res Public Health 2021;18(23):12653ArticlePubMedPMC
- 28. Darabi F, Yaseri M, Kaveh MH, Khalajabadi Farahani F, Majlessi F, Shojaeizadeh D. The effect of a theory of planned behavior-based educational intervention on sexual and reproductive health in Iranian adolescent girls: a randomized controlled trial. J Res Health Sci 2017;17(4):e00400PubMed
- 29. Salavati M, Mazaheri M, Negahban H, Sohani SM, Ebrahimian MR, Ebrahimi I, et al. Validation of a Persian-version of Knee injury and Osteoarthritis Outcome Score (KOOS) in Iranians with knee injuries. Osteoarthritis Cartilage 2008;16(10):1178-1182ArticlePubMed
- 30. Baiali Meibodi F, Mahmodi M, Hasani MD. Knowledge and practice of Kerman primarysecondary school girls on menstrual health in the academic. J Yasuj Fac Nurs Midwifery 2009;4(3-4):54-62. (Persian)
- 31. Singh MM, Devi R, Gupta SS. Awareness and health seeking behaviour of rural adolescent school girls on menstrual and reproductive health problems. Indian J Med Sci 1999;53(10):439-443PubMed
- 32. Farahani FK. Adolescents and young people’s sexual and reproductive health in Iran: a conceptual review. J Sex Res 2020;57(6):743-780ArticlePubMed
- 33. Dipti S, Chandra K. Awareness and health seeking behaviour of adolescent school girls on menstrual and reproductive health problems. Asian J Home Sci 2011;6(2):150-153
- 34. Hajivandi L, Noroozi M, Mostafavi F, Ekramzadeh M. Assessing the impact of an educational intervention program based on the theory of planned behavior on the nutritional behaviors of adolescents and young adults with PCOS in Iran: a field trial study. BMC Pediatr 2021;21(1):316ArticlePubMedPMCPDF
- 35. Lin CL, Ye Y, Lin P, Lai XL, Jin YQ, Wang X, et al. Safe sexual behavior intentions among college students: the construction of an extended theory of planned behavior. Int J Environ Res Public Health 2021;18(12):6349ArticlePubMedPMC
- 36. Ho SS, Goh TJ, Chuah AS. Perceived behavioral control as a moderator: scientists’ attitude, norms, and willingness to engage the public. PLoS One 2022;17(10):e0275643ArticlePubMedPMC
- 37. Darabi F, Kaveh MH, Majlessi F, Farahani FK, Yaseri M, Shojaeizadeh D. Effect of theory-based intervention to promote physical activity among adolescent girls: a randomized control trial. Electron Physician 2017;9(4):4238-4247ArticlePubMedPMC
- 38. Jahangiry L, Shojaeizadeh D, Abbasalizad Farhangi M, Yaseri M, Mohammad K, Najafi M, et al. Interactive web-based lifestyle intervention and metabolic syndrome: findings from the Red Ruby (a randomized controlled trial). Trials 2015;16: 418ArticlePubMedPMCPDF
- 39. Sanavi FS, Navidian A, Rakhshani F, Ansari-Moghaddam A. The effect of education on base the theory of planned behavior toward normal delivery in pregnant women with intention elective cesarean. Bimonth J Hormozgan Univ Med Sci 2014;17(6):531-539. (Persian)
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

