Physical Activity and Quality of Life
Article information
Abstract
Physical activity (PA) professionals and participants recognize enhanced quality of life (QoL) as a benefit of and motivator for PA. However, QoL measures are often problematic and rarely consider the participants'perspective. This paper focuses on recent findings from a larger project on the role of QoL in PA and health promotion. More specifically, we focus on the views of participants and potential participants to better understand the relationship of PA and QoL. In earlier stages of the project we began with a conceptual model of QoL and developed a survey. We now focus on participants' views and ask two questions: 1) what is QoL? and 2) how does PA relate to QoL? We first asked those questions of a large sample of university students and community participants as open-ended survey items, and then asked focus groups of community participants. Overall, participants' responses reflected the multidimensional, integrative QoL model, but the responses and patterns provided information that may not be picked up with typical survey measures. Findings suggest that PA contributes to multiple aspects of QoL, that social and emotional benefits are primary motivators and outcomes for participants, and that the meaning of QoL and PA benefits is subjective and contextualized, varying across individuals and settings. Programs that directly target and highlight the multiple dimensions and integrative QoL, while considering the individual participants and contexts, may enhance both PA motivation and participants' health and QoL.
INTRODUCTION
This paper focuses on physical activity (PA) and quality of life (QoL). However, focus may not be an appropriate word, as this paper takes a wide view in addressing the role of QoL in PA and health promotion. To focus somewhat, this paper presents recent findings from a larger project on QoL assessment and the role of QoL in community-based PA and health promotion programs.
To introduce the topic and provide background and context, we might ask why, what, and who questions; that is, why focus on QoL, what is QoL, and whose QoL are we focused on. The 'why' question is easy to answer: QoL is a key benefit of PA. Much research, including recent systematic reviews and meta-analyses, confirms that PA enhances QoL [1-4]. Moreover, although there is less evidence, it appears that QoL is a key motivator of PA. That is, people get into activity and stay in it because activity contributes to their QoL. Anecdotal reports from community activity programs and interview responses from a sub-sample of women in a larger study on activity and falls [5] suggest that women cite psychological values, such as maintaining cognitive function, social relations and mood, as reasons for participating. Recent research by Segar et al. [6] confirms that middle-age women are more motivated and likely to stay with activity with a focus on social psychological needs. Moreover, this view fits with most social cognitive models, and particularly with self-determination theory [7]. That is, as participants find that PA meets needs and contributes to QoL (enhances mood, social relationships, etc.) they move up the continuum toward more self-determined motivation. That positive cycle, with PA enhancing QoL, and enhanced QoL motivating participation creates a positive health cycle.
Although the research and participant reports agree that PA and QoL are related, the 'what' question is not so easily answered. Precise definitions and sound conceptual models of QoL are rare, and measures are varied. Before beginning our larger project, we reviewed the published research on PA and QoL from 2001 to 2005 to identify the current models and measures [8]. None of the 60 studies on PA/exercise and QoL explicitly cited any QoL conceptual models and the measures varied widely. The most commonly used QoL measures (e.g., SF-36) in health promotion and PA interventions were developed primarily for clinical studies and do not emphasize positive health. The American College of Sports Medicine's recent position stand on "Exercise and physical activity for older adults" summarizes evidence for benefits, including psychological and QoL benefits [9]. The evidence statement for QoL, "Although physical activity seems to be positively associated with some aspects of QoL, the precise nature of the relationship is poorly understood," is graded only D, the lowest level, while most of the 29 statements are graded A/B. Lack of conceptual frameworks and inconsistent QoL assessment may well be major reasons for the low level of evidence.
Many scholars, including those who have done the major research on physical activity and QoL, have noted that major shortcomings in our conceptual models and measures of QoL hinder both research and health promotion programs. For example, Rejeski and Mihalko [10] identified lack of precision in the definition of QoL as a barrier to consensus about the relationship between physical activity and QoL, and McAuley and Elavsky [3] argued that we cannot determine whether physical activity enhances QoL unless we can accurately operationalize and reliably measure this construct. Everyone, including researchers, health professionals and the general public, seems to understand QoL, but precise definitions are elusive. Some scholars differentiate health-related QoL, which focuses on perceived physical and mental health, from QoL. However, others find the focus on health outcomes limiting. For example, Hsieh [11] found that perceived health was not the most important factor in QoL. Similarly, we are interested in participants' views of QoL without limiting those perceptions to health outcomes; we have provided a more detailed explanation and review in our earlier report [12].
Although it is difficult to find conceptual models and definitions in the QoL literature, we can find common themes. First, nearly every reference connects QoL with positive health, and many cite the World Health Organization [13] definition, "Health is a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity." That definition, which reflects positive health and moves away from the traditional medical model, is the basis for most QoL definitions and measures. Second, virtually all definitions and models describe QoL as multidimensional, including psychological and social as well as physical domains. In addition to the themes of positive health and multidimensionality, we add that QoL is an integrative or holistic construct, and based on subjective evaluations or perceptions. Thus, in the earlier stages of our research [12], we began with a working definition of QoL that reflects positive health; quality of life is a subjective, multidimensional, integrative construct that reflects optimal well-being and positive health.
Gill et al. [12] also developed a working model to guide the development of our measure (Figure 1). That model envisions the domains of social, physical, cognitive, emotional and spiritual well-being all contributing to an integrative QoL. Also, given our focus on physical activity, we considered that physical well-being might be sub-divided into physical health, physical fitness and physical functioning. We then developed a QoL survey measure over several phases in line with that model. The resulting 32-item survey [12] fit the conceptual model, demonstrated logical relationships with physical activity, and has good psychometric properties. Still, that survey measure was derived from existing models and measures rather than from participants.
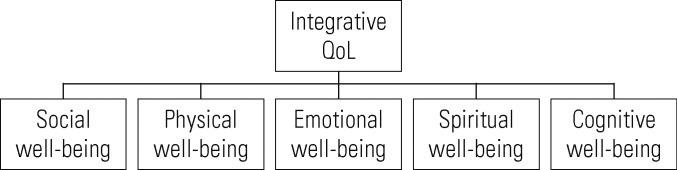
Quality of life (QoL) model.
That research helps us answer the 'what' question, and the survey fits the model and definition. However, it does not address the 'who' question-the subjective aspect of QoL. Our current work attempts to go beyond the numbers and out of the boxes to find out what real people (participants or would-be participants) see as QoL and how physical activity is related to QoL. We focus on relevance, turn to participants, and ask two questions: 1) what is QoL? and 2) how does PA relate to QoL? We first ask those questions of a large sample of university students and community participants as open-ended items on a survey, and then asked those same questions in focus groups of community participants. The following sections present our preliminary findings.
OPEN-ENDED RESPONSES OF STUDENT AND COMMUNITY PARTICIPANTS
As part of the earlier survey development phase, a sample of university students (n=142) and community participants (n=142) completed a QoL survey with two added open-ended items, "what is good QoL" and "how does PA contribute to QoL." These open-ended responses were collected with a sub-sample of the larger survey development sample. All recruitment, methods and procedures were approved by the institutional review board, and are described in detail elsewhere [12]. The community group was older (M=62.5; range, 24 to 89) than the students (M=20.8; range, 18 to 49), but similar in gender and race/ethnicity. Both groups were predominantly women (67% students, 74% community) and predominantly White (57%, 77%) with 34% and 20% African-American.
All open-ended responses to the two questions were listed in a data file and cross-checked by a second coder to ensure all responses were included. Then, similar responses were grouped together by at least 2 different coders. The research team met together to resolve discrepancies in lists and grouping to finalize the coding. It should be noted that we also asked two parallel counter questions "what is poor QoL" and "how does PA detract from QoL," and we also coded those responses. However, many participants left those items blank, the limited responses did not add to the findings, and thus are not reported.
What is Quality of Life? Open-ended Survey Findings
Both student and community participants' responses on 'good QoL' encompassed all domains of QoL, but certain domains and specific responses were stronger contributors, and patterns differed between the two groups. As Table 1, which gives the frequencies of responses in the major categories, shows, physical health is important, but QoL is much more than physical. Both student and community groups gave similar high numbers of responses that fit the social category (56, 54) and physical health (66, 64) domain. For the emotional category, students gave markedly more responses (77 vs. 31). For physical function/activities of daily living (ADL), community participants gave more responses than did students (65 vs. 19). That's logical, given that many community participants were in senior activities, but it is notable that students also gave responses indicating that physical functioning was an important part of QoL. Responses that reflected the cognitive and spiritual domains were also given by both students and community participants.

What is quality of life: participant responses
Several participants also gave responses in the environmental category, such as having what you need. Notably almost no one left the open-ended item blank even though the item was at the end of a lengthy survey. We did code and analyze the counter question, "what is poor QoL" but the responses were fewer and generally simply a reverse of the responses to 'good QoL.' Overall, participants' responses reflected the multidimensional QoL model underlying the survey. However, the varied responses and patterns suggest that the meaning of QoL varies across groups and individuals in ways that may not be picked up with survey measures.
Physical Activity and Quality of Life: Open-ended Survey Findings
The same sample responded to open-ended items asking how PA contributes to QoL and detracts from QoL. As Table 2 shows, nearly all participants reported positive contributions with less than 15% of both groups leaving the open-ended item blank. Clearly, participants see PA as contributing to positive health and QoL. As expected, physical activity contributes to the physical domain, but that's not all. Both groups reported PA contributions in all QoL domains, with the most responses under physical health (44, 37) and emotion/mood (44, 43). Patterns of specific responses within those domains differed. For example, under the emotion domain, students reported more stress relief. Within the physical domain, both groups gave many responses reflecting physical health, but community participants reported more ADL contributions; both groups reported similar numbers of responses reflecting physical fitness, but students cited staying fit whereas community participants cited flexibility and strength.
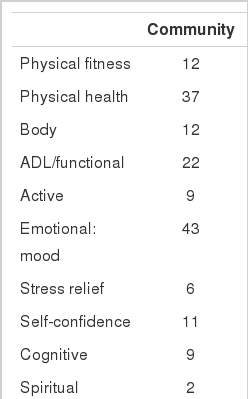
How does physical activity contribute to quality of life: participant responses
The overwhelming response to the counter question "does PA detract from QoL" was a clear 'no' with very few participants responding with anything else. Both students and community participants clearly see PA as contributing to QoL. Not only did both groups cite clear contributions to the physical domain, but similar large numbers reported contributions to the emotional domain, and several reported contributions to social, cognitive and even the spiritual domain. Of particular interest, a notable number gave responses that explicitly reflect an integrative QoL.
COMMUNITY FOCUS GROUP FINDINGS
As an extension of the survey research, this phase of the project more directly focuses on the meaning of QoL from the perspective of participants in community programs. The focus group study was conducted after the survey development phase, and received separate approval from the university human subjects institutional review board. Through contacts with community programs, six different focus groups of 5 to 7 participants were formed. Participation was voluntary and confidential and all participants provided informed consent. Two groups came from one church, and both groups were young to middle-aged (age 24 to 48) Black women. The other four groups were predominantly White women, but each was distinct, including novice women runners in a training program (age 33 to 55), a clogging group (age 18 to 55, including the only man in the focus groups), an activity program for women with fibromyalgia (age 54 to 83), and a YMCA senior fitness class (age 65 to 73).
The focus group interviews were semi-structured, and the main guiding questions asked of the focus groups were, "what is QoL" and "how does PA relate to QoL." Facilitators were graduate students with experience in qualitative methods and focus groups. Sessions were audio-taped and transcribed; transcripts were reviewed to identify responses related to the meaning of QoL and its relationship to PA, then listed for coding. At this point our analyses are preliminary, but provide a glimpse into the meaning of QoL and PA for participants.
What is Quality of Life? Focus Group Findings
Figure 2 gives a summary of the responses in QoL categories. However, the numbers do not really tell us what QoL means to the participants. Several responses were common to all the groups, but each focus group also provided some unique responses, highlighting the subjective nature of QoL, and also suggesting social-contextual influences. All of the focus groups cited responses that reflected multiple QoL domains (e.g., physical, social, and emotional) and all emphasized balance or integration of different aspects of QoL. Common responses from all groups included enjoying life, able to do things, social connections, and good health. Responses reflecting the spiritual domain were cited in several groups, but most notably in the two groups that came from the church. The senior group emphasized cognitive skills and independence, and the fibromyalgia group emphasized relief of symptoms. As with the open-ended survey responses, focus group responses reflected multidimensional QoL. However, varying patterns also suggest that the meaning of QoL varies across groups and individuals in ways that may not be picked up with survey measures.
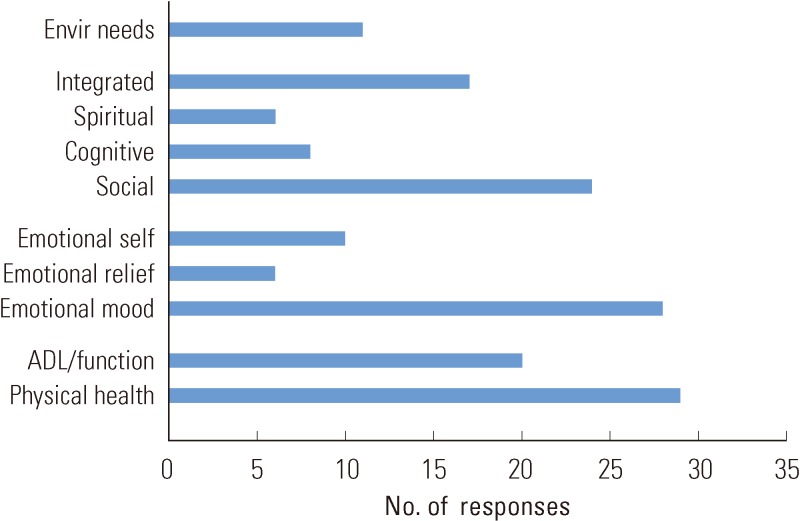
What is quality of life? Focus group responses. ADL, activities of daily living.
Focus groups clearly told us that the physical and emotion domains were key components of QoL. Physical health was cited in all groups, and the ability to stay active and function is a big factor for participants. As one participant stated, QoL is "...ability to do everything that you want to do in life." The social is clearly very important, and groups also mentioned cognitive and spiritual dimensions of QoL. Notably, several comments reflected a balanced or integrative QoL. Participants clearly indicated that all components (physical, social, emotional, cognitive, and spiritual) play a part. As one stated, "I think it's a balance of all those things, especially being able to enjoy yourself, have a level of health-not only physically... emotionally, and so that you can have that balance..." As reflected in the focus group findings, QoL is clearly positive, multidimensional and integrative. And, the meaning of QoL is subjective and socially or contextually situated.
Physical Activity and Quality of Life: Focus Group Findings
As with the responses to the meaning of QoL, groups expressed many similar responses, while also presenting some unique perspectives (Figure 3). Of course, participants cited physical benefits, and comments referred to physical health, body, energy, and particularly the ability to do things and be active. One stated, "I have the energy to do all those things I want to do." Another comment connected physical and emotional benefits, suggesting that physical changes give confidence, "You can do all those things. So, just get up and do it."
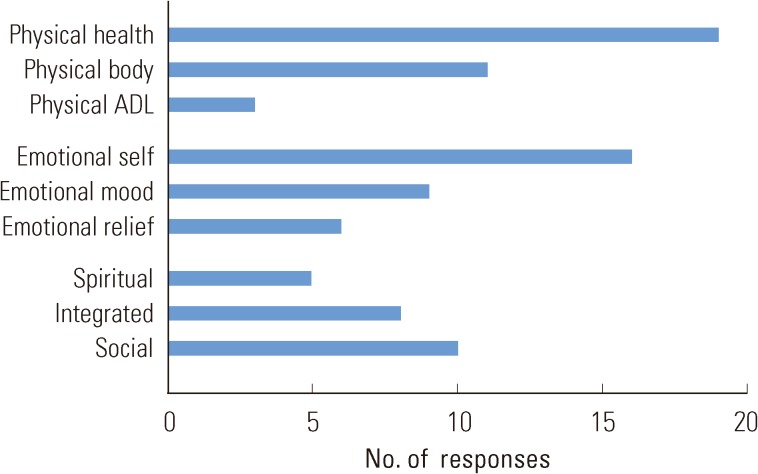
Physical activity contributions to quality of life: focus group responses. ADL, activities of daily living.
All groups cited social and emotional benefits as well as physical, and indeed, often emphasized social or emotional benefits over physical. For example, although the women runners were in a training program for a women-only 5-km run, almost no responses reflected physical condition or abilities; instead they cited confidence, energy, stress relief, time management and feeling better. Similarly, the cloggers, who were in a group purposely formed for the physical activity of clogging, clearly agreed that social benefits were primary.
Physical activity clearly contributes to emotional well-being for the participants in several ways. Several comments reflected PA for self-confidence, self-discipline and self-acceptance, including "It motivated me to be OK with myself" and "We gain lots of dignity." PA for enhanced mood and stress relief was another consistent theme under the emotional category. Participants indicated that PA improved their emotional state with comments including, "If I'm stressed, I go to the gym...I can work this off," and "Running in the morning prepares the whole day for me."
Interestingly, social contributions were cited several times as participants reported that PA helps them interact with different people, develop camaraderie, and improve family relationships. Contributions to the cognitive and even the spiritual domain were also cited. For example, one participant stated, "I feel closer to God...when I'm physically active," and another commented, "If I'd been inside on the couch, I wouldn't have paid any attention to the clouds and the sun and the trees and the nice breeze."
Again, many responses emphasized balance or integration of different aspects of QoL in relation to PA. When specifically asked about relative contributions many responded that that they could not rank the domains or separate them. As one participant stated, "I think exercise affects every dimension of your life" and another added, "...all go together and impact each other, blended together."
CONCLUSION
The views of our participants on QoL and the PA-QoL relationship reflect the model, survey results, and literature, but adding the subjective (real people) views to our objective measures and results gives a much richer picture. Both the open-ended responses and focus group findings suggest that Qol reflects positive health and is multidimensional, subjective, and integrative. It is also quite clear that physical activity contributes to all aspects of QoL-not just the physical. Indeed, the social and emotional benefits may be the primary motivators for community participants. Considering participants' subjective views tell us that the meaning of QoL and PA contributions varies across people and contexts. It should be noted that although our findings provide insights, our study, and particularly our focus group findings are limited in several ways. At this point, our analyses are preliminary and lacking in depth. Our focus group participants were nearly all women and from groups with very specific purposes and contexts. Those specific contexts contribute to the findings and that individualizing and contextualizing aspect has implications for research and professional practice.
More specifically, the findings suggest that we might target QoL to enhance motivation and make sure that PA truly contributes to QoL for participants. Rather than focus on traditional physical fitness outcomes, we can target QoL outcomes, and specifically target outcomes that are important and meaningful for participants and potential participants. Even though physical benefits are important, participants rarely mention the typical fitness measures that we often target with typical frequency, intensity, and time prescriptions. Indeed, emotional, social even physical health goals of many participants may be lost in focusing on training criteria.
In as recent research article, Segar et al. [6] concluded that we could better promote sustainable PA participation by rebranding exercise as a primary way individuals can enhance the quality of their daily lives. I agree. And, I would add that we can better do that if we ask the 'who' question and consider that subjective, contextualized meaning of QoL and its relationship to physical activity for our participants and potential participants. Additional studies, with participants in different activity settings and across differing cultural contexts, could add richer insights.
One of our participants summed up our conclusion eloquently, "I think we should still have recess." Recess - that implies PA that is clearly positive with emotional, social and perhaps spiritual connotations - and lots of fun. Recess is physical activity for QoL. We should all have more recess in our PA programs and in our lives.
Notes
The authors have no conflicts of interest with the material presented in this paper.