Factors Affecting Public Prejudice and Social Distance on Mental Illness: Analysis of Contextual Effect by Multi-level Analysis
Article information
Abstract
Objectives
While there have been many quantitative studies on the public's attitude towards mental illnesses, it is hard to find quantitative study which focused on the contextual effect on the public's attitude. The purpose of this study was to identify factors that affect the public's beliefs and attitudes including contextual effects.
Methods
We analyzed survey on the public's beliefs and attitudes towards mental illness in Korea with multi-level analysis. We analyzed the public's beliefs and attitudes in terms of prejudice as an intermediate outcome and social distance as a final outcome. Then, we focused on the associations of factors, which were individual and regional socio-economic factors, familiarity, and knowledge based on the comparison of the intermediate and final outcomes.
Results
Prejudice was not explained by regional variables but was only correlated with individual factors. Prejudice increased with age and decreased by high education level. However, social distance controlling for prejudice increased in females, in people with a high education level, and in regions with a high education level and a high proportion of the old. Therefore, social distance without controlling for prejudice increased in females, in the elderly, in highly educated people, and in regions with a high education and aged community.
Conclusions
The result of the multi-level analysis for the regional variables suggests that social distance for mental illness are not only determined by individual factors but also influenced by the surroundings so that it could be tackled sufficiently with appropriate considering of the relevant regional context with individual characteristics.
INTRODUCTION
Public prejudice and social distance towards mental illness have impeded early treatment and early recovery of the psychiatric patients through optimal utilization of mental health services [1-4]. Better understanding of the current status and cause of public prejudice and social distance towards mental illness could benefit the patients via improving opportunity to get proper treatment. Relevant discussion and policy amendment, as well as new agendas to help fight the stigma towards mental illnesses have been increasing recently in Korea [5,6].
Personal beliefs and attitudes towards mental illnesses are not only related to individual characteristics but also highly influenced by their surrounding regional context. Structural discrimination like institutional racism as well as individual discrimination [7] shows these two simultaneously working dimensions. Regional context such as age structure, regional level of education, and regional level of income may influence individual attitudes within the region. In addition, many public campaigns and education programs have been committed at the regional level. Such public intervention programs, therefore, would be benefitted from better understanding of structural reasons and pathways as well as individual knowledge and familiarity towards mental illness. However previous studies have not tackled the contextual effect simultaneously with individual factors even though some research investigated individual socio-demographic characteristics [8]. Other previous studies on attitudes towards mental illness in Korea were based on either non-nationally representative dataset or on limited range of factors on attitude [9,10], and most of the studies on the public attitude towards mental illnesses have been accomplished in Western countries [11]. Thus, we examined the recent trends of the public beliefs and attitudes towards mental illnesses and explored factors that affect the public's beliefs and attitudes including contextual effects in Korea.
METHODS
I. Study Population
Nationwide telephone survey on the public's beliefs and attitudes towards mental illnesses in Korea from 2007 to 2010 were used for the study. This survey, which adapted structured questionnaire, represents the whole population from 15 to 69 years of age in Korea. The survey selected people with a random sampling method, and the response rate of these telephone surveys were 29.5% to 33.4% except for 2007, which lacked data on the response rate. A total of 4369 individuals were interviewed from 2007 to 2010. Of those individuals, 312 were excluded since they lacked sufficient information. We finally analyzed 4,057 individuals who answered the questionnaire completely.
II. Conceptual Model
Individual and regional socio-economic factors and social distance models were used, which suggested a consecutive order of familiarity (knowledge), prejudice, and social distance reported by Corrigan et al. [12] and Moon et al. [8] to determine the factors influencing the public's attitude towards mental illnesses. The public's beliefs and attitudes in terms of prejudice were analyzed as intermediate outcomes and social distance as final outcomes (Figure 1). The model for social distance was divided again into two models: 1) social distance with the prejudice variable and 2) social distance without the prejudice variable. Therefore, three models were made to explain prejudice (model A), social distance (model B), and social distance without prejudice variable (model C). Prejudice and social distance are different apparently in concept even though these are closely correlated. Prejudice questions investigate people's wrong perception but social distance questions investigate discriminative attitude. So we can analyze causes of social distance separately to social distance derived wrong perception and social distance unrelated wrong perception by controlling prejudice on social distance in model B. Almost previous studies for public attitude to mental illness analyzed prejudice or social distance only as far as we reviewed related articles. Then each model divided to two models again to explain regional environment. The first model included year and individual level variables. Second model include regional variables as well as year and individual variables to determine the social effect. Finally, we compared the both individual and regional socio-economic factors, familiarity, and knowledge, between the models, intermediate and final outcomes.

Concept of the research model.
A. Definition of variables
Individual socio-economic factors in this research included age, sex, education level, and economic level variables. The age was grouped as follows: under 30 group, 30 to 39, 40 to 49, 50 to 59, and 60 or more. The education level was divided into three subgroups: 1) middle school graduation or less, 2) high school, and 3) college entrance or more. The economic level variable was a subjective self-rating grade and divided into three groups: low, middle, and high.
Regional socio-economic variables related to 16 provinces were investigated from the database of the Bureau of Statistics in Korea. Regional variables were economic level, education level, welfare level, and age structure comparable with individual variables to figure out pure regional effect. We used the gross regional domestic product per person as the regional economic level. The regional proportion of people whose educational attainment was college or more was used as the regional education level. The proportion of welfare spending of the total budget of the province was used as the regional welfare level. The proportion of people aged 65 and over in the province was used as the regional age structure.
We followed previous study for defining individual familiarity, knowledge, prejudice, and social distance from the survey on the public's beliefs and attitudes towards mental illnesses in Korea [8]. Moon et al. [8] implement survey questionnaire for Korean with review of similar surveys in other countries and consultation to psychiatrist for face-validity. We discarded one prejudice question about hospitalization in analysis because this question modified after 2008 and used total 16 questions for public knowledge, familiarity, prejudice and social distance for analysis (Appendix 1).
Knowledge was defined as having knowledge on the cause, prevalence, and behavioral characteristics of mental illness. Familiarity was defined as experience with mental illness by someone close or themselves and recognition of regional mental health programs. Prejudice was defined as adopting public stereotypes and emotional reactions. Social distance was defined as behavioral characteristics in terms of prejudice. An average 5-grade Likert scale was used with 4 questions for social distance. An average 5-grade Likert scale was used with 7 questions for prejudice. Knowledge was measured with an average 5-grade Likert scale with 3 questions. Familiarity was measured by 2 questions and a 0-2 scale was used. High score of familiarity, knowledge, prejudice and social distance means high level of familiarity, knowledge, prejudice and social distance.
B. Statistical analysis
Trends for familiarity, knowledge, prejudice, and social distance from 2007 to 2010 were analyzed. The relationship of prejudice and social distance with the other factors were analyzed using multi-level regressions with three level modeling (year, region, and individual level).
RESULTS
There were 1825 (45.0%) people whose educational attainment was college or more. A total of 658 (16.2%) people considered themselves as a low income person, and 1107 (27.3%) considered themselves as a high income person. Females had a high social distance of 2.697 than that of males at 2.553. Prejudice and social distance became worse as age got older. With increasing education level, knowledge and familiarity increased and prejudice decreased, but social distance did not change much. People with high economic status had low familiarity and knowledge compared to people with low economic status, and prejudice increased when economic level increased but social distance was not so different (Table 1).
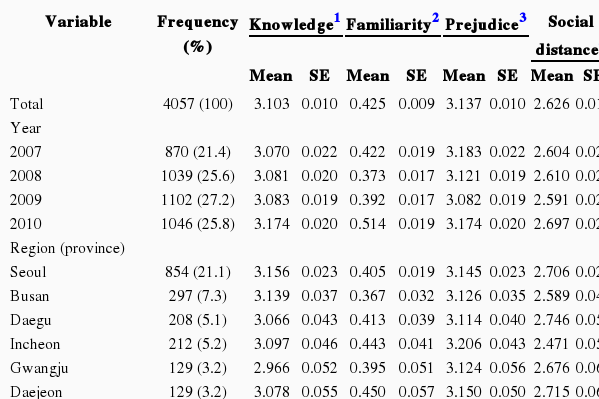
Baseline characteristics of the study subjects
Familiarity increased via rebounding after decreasing in 2008 since 2007 (p<0.001). Knowledge also increased in 2010 compared to 2009 (p=0.001) after the period of plateau in 2007 to 2008 even though the degree of increase was less than that of the familiarity (Figure 2, Table 1). However, prejudice and social distance as the beliefs and attitudes towards mental illness also increased in 2010 compared to 2009 (p=0.001, 0.002) (Figure 3, Table 1).

Recent trends in public knowledge and familiarity for mental illness.

Recent trends in the public's beliefs and attitudes towards mental illness.
Table 2 shows the results of the multi-level analysis for prejudice and social distance, using two levels model 1 included year-level and individual-level variables and region-level variables were added to the variables of model 1 in the model 2. The likelihood ratio test for social distance (model B) showed that adding the regional variables resulted in a statistically significant improvement in model fit (Δ-2LL(log-likelihood)=13.94, d.f.(degree of ferrdom)=4, p=0.007). The model for prejudice did not show any improvement in the model fit when regional variables were appended (Δ-2LL=2.92, d.f.=4, p=0.571). The social distance model without the prejudice variable (model C) showed significant improvements in model 2, also (Δ-2LL=13.24, d.f.=4, p=0.01).

Results of multi-level analysis for prejudice, social distance and social distance without prejudice variable
Prejudice was not explained by the regional variable, but only correlated with the individual factors. Prejudice increased with age and decreased with education level, knowledge, and familiarity. Sex and income were not related to prejudice.
However, in the social distance, females and a high regional proportion of college educational attainment, regional proportion of people aged 65 and over, which was not related with prejudice, showed association with social distance (p<0.001, p=0.003, and p=0.032). Age was not related to social distance except for the 30 to 39 group. Social distance increased in the college-or-more educational attainment, which had a decreasing effect on prejudice (p=0.001). Income was not related with social distance like prejudice. Knowledge and familiarity was related negatively with social distance (both p<0.001). Social distance increased with increases in prejudice (p<0.001).
When social distance model was analyzed without the prejudice, sex, which was insignificant in the prejudice model but significant in the social distance model, was significant. Age that was positively correlated with prejudice but insignificant in the social distance model except for the 30 to 39 age group, but its regression coefficients decreased more than that of the social distance model with the prejudice because the coefficients had adverse directions between models A and B and canceled each other's effect out. Familiarity and knowledge, which had negative correlations in both model A and B, was intensified by adding each effect. Educational level had a negative correlation in model A but a positive correlation in model B; therefore, its coefficient was canceled out and became small and insignificant in model C. Income was not correlated in any model; thus, it was not significant in model C too.
DISCUSSION
We examined the recent trends on the familiarity, knowledge, prejudice, and social distance towards mental illnesses in Korea and showed the related factors of prejudice as an intermediate outcome and social distance as outcome.
No regional variable was significant in explaining the prejudice; however, social distance was significantly increased as regional education level and proportion of the old increased. This shows that individual social distance on mental illness is not only determined by individual factors but also influenced by the surroundings. In other words, social distance differs from prejudice in terms of influence of contextual characteristics. If there are two areas, area A and B, and their difference in proportion of people whose educational attainment was college or more is 20%, then persons who have identical in individual variable has difference in social distance around 0.24. This degree is bigger than effect of increasing 1 point in individual knowledge and familiarity.
The results of analysis for the individual variables suggest that sex, age, and education level have effects both on prejudice or social distance. Concerning gender, previous studies revealed inconsistent finding on social distance and the relationship in previous studies varied: no association, or positive, or negative correlation [8,13-23]. Unlike the previous studies, in this study, females did not differ from male with regard to explaining prejudice but social distance was significantly different between males and females after controlling covariates. This may tell the possibility that gender may have an effect on discriminative behavior. Social distance increased with age in model C in this study, and this finding is in line with previous studies [13-16,18-24]. However, the social distance model with the prejudice (model B) did not show any association with age. This means the influence of age on social distance came through prejudice, which may tell the possibility of elimination of age effect on social distance by proper education. Social distance decreased with a high education level in many previous studies while some reported no associations [13-16,18-24]. In this study, education level also had no association with social distance in model C while the results in models A and B reveal the education level has a very significant effect on both prejudice and social distance, which means the results in model C were cancelled-out effects. These findings suggest that a high education level reduces prejudice but makes social distance increase to the same extent; therefore, social distance can be misunderstood as if it had no association with educational attainment.
We analyzed causes of social distance separately to social distance derived wrong perception, prejudice, and social distance unrelated wrong perception by separating three models. We expect this separation of model can provide some policy implications which can intervene in public attitude more precisely by figure out detailed causes of social distance. For example, we can adopt public campaign to correct prejudice to lowly educated people and that can make them to have low social distance. However that is not enough to highly educated people because their social distance is less related with prejudice than lowly educated people. So we should focus campaign for reducing social distance itself as well as prejudice to highly educated people.
There is a limitation of this study which needs to be addressed. Even though a random sampling method was used, this study, based on telephone survey with a response rate around 30%, could not be free of selection bias.
Considering the community intervention programs for the alleviation of social discrimination, further studies to determine the mediating factor between the regional education level, regional proportion of the old and social distance are needy. In addition, comparison between the regional contextual effects in Korea with other cultural contexts from various western countries is necessary.
In conclusion, social distance has a different association with regional context from prejudice, which suggests that social distance is not just a matter in the individual level so that we could tackle structural discrimination to improve the public's attitude.
Notes
The authors have no conflicts of interest with the material presented in this paper.
This article is available at http://jpmph.org/.
