Social Determinants of Smoking Behavior: The Healthy Twin Study, Korea
Article information
Abstract
Objectives
The purpose of this study was to identify any influence of socioeconomic status on smoking and smoking cessation in a situation where genetic factors are controlled.
Methods
The sample for this study was 2502 members of the twins and families cohort who participated in the Korean Healthy Twins Study from 2005 to 2009. Groups of brothers or sisters, including twins and fraternal twins, were compared in terms of smoking and smoking cessation behaviors according to differences in socioeconomic status and gender.
Results
In a situation with complete control of genetic factors, results showed that the daily smoking amount, cumulative smoking amount, and dependence on nicotine decreased with higher-status occupations, and the rate of smoking and amount of cumulative smoking decreased with higher levels of education. Regarding smoking cessation behavior, a higher level of education was associated with a lower smoking cessation rate, and no significant gender differences were found.
Conclusions
Environmental factors had a stronger influence on smoking behavior than did genetic factors. Genetic factors had greater influence on smoking cessation than did environmental factors; however, this requires verification in further studies.
INTRODUCTION
According to current theories on health, factors that can affect human health include socioeconomic level, environmental causes, biological causes including genetic causes, individual health-related behaviors, and the medical system of a country [1]. Individual health-related factors include smoking, drinking, exercise, eating habits, and sleeping habits [2]; of these, smoking is especially important. According to the World Health Organization (WHO), in the year 2009, 5 million people worldwide die from smoking-related causes every year, and smoking is one of the most important preventable risks to human health [3-5].
One environmental influence on human health is socioeconomic status (education level, income level, occupation), as has been reported in previous studies [6-8]. Differing socioeconomic levels are associated with different smoking behaviors; in lower socioeconomic levels, people have a higher tendency to smoke [9-14]. In Korea, low socioeconomic status is associated with risky smoking-related behaviors [15-18] and with a low rate of success rate in quitting smoking [15,17].
Genetic factors can also affect smoking behaviors, and previous studies have shown that not only nicotine addiction but also behaviors related to smoking have a genetic component [19-23]. These findings show that socioeconomic status, other environmental causes, and genetic causes are all associated with smoking, but most research conducted in Korea has focused on the relationship between socioeconomic factors and smoking. There is no previous report on smoking-related environmental and genetic causes in twins. The effects of genetic factors on an individual's health differ according to population group [24]. Thus, it is important to examine how socioeconomic level is related to smoking among Korean subjects when genetic factors are controlled.
Based on Korea's twin cohort data, in this study, we examined how socioeconomic factors affect smoking behavior (smoking rate, daily smoking amount, cumulative smoking amount), efforts to stop smoking and the success of those efforts, and the degree to which a smoker is dependent on nicotine.
METHODS
I. Participants
This research was conducted from April 2005 to December 2009 with twins and their family members (n=2860) from Samsung Medical Center and Inje University Busan Paik Hospital who volunteered to participate in this study. Identical twins over the age of 30 were selected, and these twins'first-degree relatives, non-identical twins with or without family members, and 4th-degree blood relationships were included if the participants agreed; family members based on marriage relationships (except for parents) were not included in this research. A questionnaire was used to collect information on diet and exercise, family history of disease, smoking, drinking, changes in the environment, and socioeconomic status. In this study, we used only the questionnaire data related to smoking and socioeconomic level. Data were collected from 2502 people (358 people refused to complete the questionnaire). These subjects included twin brother and sister pairs (males 332 [166 pairs], females 556 [278 pairs]) and siblings pairs including a twin (males 732 [366 pairs], and females 1152 [576 pairs]).
II. Measures
Zygosity was confirmed using 16 short tandem repeat (STR) markers (15 autosomal STR markers and 1 sex-determining marker) in 67% of the twins, and zygosity data from previous research were available for the rest [25]. Variables showing socioeconomic level, income level, educational level, and occupation used existing literature as a reference [6,7,15]. For income, equivalized household income was calculated as the square root of the household income divided by the number of people in the household. Based on this figure, subjects were divided into quartiles, and four income groups were established: low income, ≤25%; middle income, the two quartiles comprising 25% to 75%; and high income, >75% [26-28]. Education level was classified in there levels: middle school graduation or less, high school graduation, and college graduation and above. For occupation, Statistics Korea's standard occupation classification table was used based on data that subjects provided, and the occupations were classified into non-manual and manual workers. People whose occupations were manager (public and high-ranking officer in a company; administration and management support manager; expert service management position and its manager; construction, electricity, and production-related management position; sale and customer service management position), specialist and related profession, and white-collar workers were classified as non-manual workers. People whose occupations were service worker, sales-related worker, and simple labor workers were characterized as manual workers [26,28,29]. People who did not fit in either category were classified as "other" (housekeepers, students, and fully retired); data from these subjects were excluded from further analyses.
Variables related to smoking behavior were smoking status (present smoker: someone who is smoking at the present and who has smoked more than 400 cigarettes; past smoker: someone who does not smoke now but who has smoked more than 400 cigarettes; non-smoker: someone who has never smoked before or a smoker who has smoked fewer than 400 cigarettes) [30], daily smoking amount (cigarettes/d), cumulative smoking amount (packs/y), and nicotine dependence (assessed using the Fagerstrom test for nicotine dependence). To find the extent of nicotine dependence, we used data that the participants provided in the Korea Twin Study using a questionnaire from previous research [31]. Variables related to smoking cessation were attempts to quit smoking (tried or did not try) and success in quitting (continuous non-smoking for 6 months or longer).
III. Statistical Analyses
Based on previous studies [32,33], data were divided into a sibling group and a monozygotic twin group (MZ). All subject variables are presented as frequencies and percentages; daily smoking amount, cumulative smoking amount, and nicotine dependence are presented as means with standard deviations. In the remaining analyses, the analysis was done with common targets only, with exclusion of missing values (the process excluded missing-value targeted subjects with siblings or twins if one twin was missing, and those data were not included in the analysis). For smoking-related variables, data were available for 937 pairs of siblings including twins (male, 365 pairs; females, 572 pairs) and 442 pairs of MZ twins (male, 165 pairs; female, 277 pairs). For non-smoking-related variables, data were available for 909 pairs of siblings including twins (male, 341 pairs; females, 568 pairs) and 436 pairs of MZ twins (males, 161 pairs; females, 275 pairs). In sibling pairs with twins included and in every pair of MZ twins (sibling pairs were selected in the same sex siblings), to assess differences in smoking behavior according to socioeconomic level, differences in smoking rate were calculated using conditional logistics, and odds ratios (95% confidence interval [CI]) were used to indicate differences in associations between smoking rate and socioeconomic levels between the pairs. Differences in daily smoking amount, cumulative smoking amount, and nicotine dependence were observed, and differences in smoking behavior values were calculated by regression analysis and are expressed in terms of beta values (95% CI) when socioeconomic status varied by one grade.
To observe changes in smoking cessation according to socioeconomic level, we controlled for elements such as age, gender, and drinking habits (yes or no, because smoking cessation variables were binary) and then assessed differences in the rate of smoking cessation attempts and successes according to socioeconomic status. In the siblings group that includes twins and in the MZ twin group, we used conditional logistic regression to compare the smoking-cessation attempt rate (failure to quit smoking for 6 months) and smoking-cessation success rate (success in quitting smoking for 6 months) to compare sibling pairs (female siblings and male siblings paired together) according to socioeconomic level. Because it was possible that the smoking rate would differ according to gender, the analysis was done separately by gender. All analyses were done with SAS version 9.2 (SAS Inc., Cary, NC, USA).
RESULTS
Table 1 shows the data on socioeconomic level and smoking-related variables. The sibling group including twins contained 732 males (366 pairs; mean age, 39.72±8.21 years) and 1152 females (576 pairs; mean age, 39.04±7.83 years), and the monozygotic twin group had 322 males (166 pairs; mean age, 39.15±7.50 years) and 556 females (278 pairs; mean age 37.78±7.05 years). In both the siblings group and the monozygotic twin group, males occupied majorities in the higher levels of education and income. In terms of occupation, more females than males were classified in the "others"group including many women who were housewives. More males than females reported occupations categorized as non-manual work. In the sibling group (twins included) 52.05% were current smokers, and 48.64% of subjects in the monozygotic twin group were current smokers. The daily smoking amount, the cumulative smoking amount, and nicotine dependence were higher in males than in females.
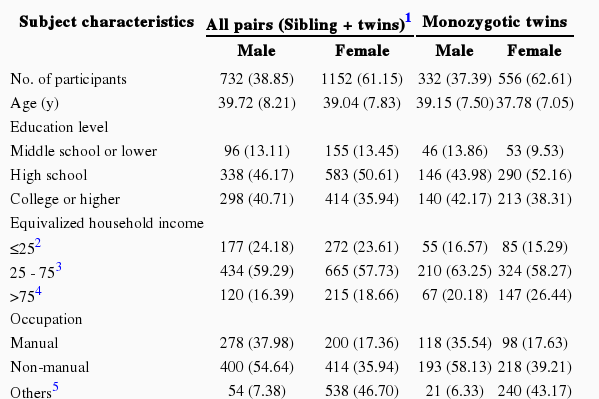
Characteristics of study population from the Healthy Twin Study
Table 2 shows changes in smoking behavior according to socioeconomic level with genetic causes controlled. First, overall, single-grade increases in education level, income level, and occupation level resulted in no statistical difference in rate of smoking, daily smoking amount, or cumulative smoking amount. However, in the case of monozygotic twins, whose genetic factors were 100% controlled, when education level increased by one grade, smoking decreased by 0.67 times (95% CI, 0.51 to 0.93), and cumulative smoking decreased by 2.9 fold (95% CI, -4.77 to -1.95; this difference was statistically significant), but income level was not significantly associated with smoking-related behaviors. With respect to occupation level, an increase of one grade in occupation level was associated with a 2.48-fold decrease in daily smoking amount (95% CI, -3.52 to -1.44), and cumulative smoking amount decreased by 8.7 fold (95% CI, -10.29 to -7.11); these differences were statistically significant.
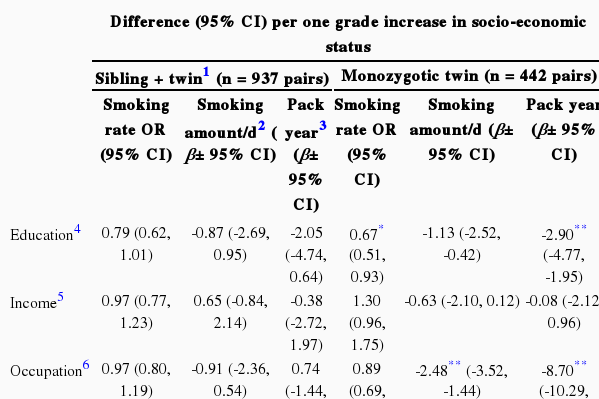
Smoking indices and social determinants in sibling and monozygotic twin pairs (analyses between withinpair differences)
Table 3 shows changes in smoking-cessation behavior according to socioeconomic level, controlling for genetic factors. Within each gender, when education level and income level increased by one grade, the odds ratio for nicotine dependence dropped by 0.70 times (95% CI, -1.28 to -0.11) and increased 0.65 times (95% CI, 0.15 to 0.96), respectively (statistically significant differences), but no similar result was found for stop-smoking attempts or stop-smoking success. When occupation level increased by one grade, the odds ratio for stop-smoking success was 0.45 times higher (95% CI, 0.21 to 0.97); this was a statistically significant difference. However, no statistically significant difference was found in the stop-smoking attempt rate or in the nicotine dependence rate. When income level and occupation level increased by one grade, the odds ratios for nicotine dependence were 0.52 times higher (95% CI, 0.09 to 0.74) and 1.29 times lower (95% CI, -1.80 to -1.03), respectively (statistically significant differences), but the stop-smoking attempt rate and success rate were not significantly different.

Smoking cessation behaviors according to social determinants in sibling and monozygotic twin pairs (analyses by pair-wise differences)
Table 4 shows changes in smoking behavior by gender according to differences in socioeconomic status while controlling for genetic factors. First, when considering the comparisons between same-sex siblings including twins, the results were not very different from Table 2, where male and females combined were analyzed. The exception was for males, where if the education level increased by one grade, the smoking rate was 0.62 times (95% CI, 0.45 to 0.84) lower. However, in the case of females, there were no statistically significant results. Second, considering the results for identical twins, males showed the same results as in Table 2, but the outcomes were statistically more significant. However, in the case of females, there was no statistically significant result even in identical twins.
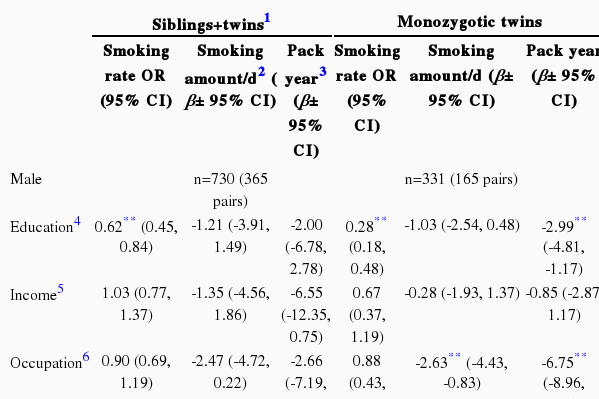
Gender-specific smoking behavior patterns and social determinants in sibling pairs and twin pairs (analyses by within-pair differences in the two factors)
Table 5 shows smoking-cessation behavior by gender according to socioeconomic status with genetic factors controlled. First, considering the results for same-sex siblings, including twins, in the case of males, when occupation level increased by one grade, the smoking-cessation success rate was 1.62 times higher (95% CI, 1.09 to 2.42), similar to results shown in Table 3, which combines data from males and females. However, unlike the result in Table 3, the nicotine dependence score was not significantly associated with socioeconomic status. In the case of females, there was no statistically significant result. Second, considering the results for identical twins, in the case of males, except for the fact that if occupation level increased by one grade, then nicotine dependence decreased -0.72 times (95% CI, -1.31 to -0.13), the results were not statistically significant, and in case of females, there was no statistically significant result in any variable.
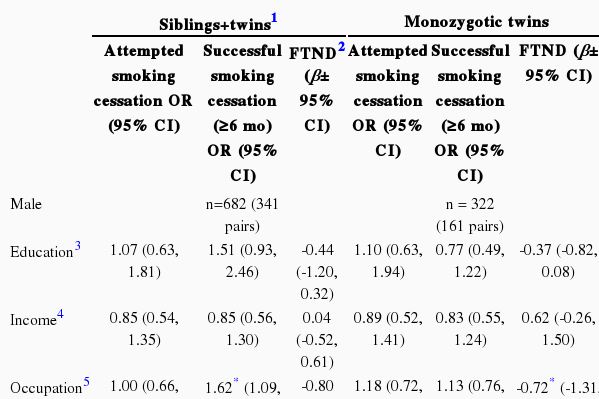
Gender-specific smoking-cessation behavior and social determinants in sibling and twin pairs (using within-pair differences)
DISCUSSION
This research was conducted to assess differences in smoking behavior and smoking-cessation behavior according to differences in socioeconomic level, based on data from the Korean twins' cohort. Data were analyzed for the siblings group including twins, which controlled for genetic factors to some degree, as well as for MZ twins, which controlled completely for genetic factors.
After analyzing identical twins, whose genetic factors were controlled 100%, the socioeconomic factor that apparently had the strongest effect on daily smoking amount, cumulative smoking amount, and nicotine dependence was occupation. Also, the result showing that a higher level of education is associated with a lower rate of smoking is consistent with the existing literature [13]. Despite previous reports that genetic factors are related to smoking behavior, these results indicate that socioeconomic factors can have greater effects than genetic factors.
The socioeconomic factor that had the greatest effect on stop-smoking behavior was education level. Surprisingly, in this research, as the education level got higher, the stop-smoking success rate decreased. In a previous study, an analysis that controlled only for age showed that as education level increased, the rate of quitting smoking also increased. However, when other socioeconomic factors were controlled, the results showed no relationship between increased education level and success in quitting smoking [15,34]. In addition to the fact that socioeconomic factors identified in other research were controlled in the present study, our finding showing a decrease in the quit-smoking success rate as education level increased may also be due to the fact that in studying twins, not only are genetic factors a 100% match but also the environment inside the womb and childhood environmental factors such as having grown up and shared many things together are very similar. These results can be interpreted as showing that the effect of education level is much greater than that of genetic factors on stop-smoking behavior. However, in the gender-stratified result, the effect of education level was not as clear in either gender. Thus, further research is required to address this more specifically.
Additionally, the association between socioeconomic level and both smoking and stop-smoking behaviors was similar in the sibling group to that in identical twins. In the case of females, we found no statistically significant differences, although females tend to have much lower smoking rates than do males generally, and there is a possibility that smoking among women was under-reported.
Since 2004, perhaps in response to price increases for cigarettes and other national attempts to encourage people to quit smoking, the smoking rate among Korean males has been steadily decreasing, and in 2010, it was 39.6%. However, based on a 2009 investigation, the rate in Korea was still high compared with that in the USA (17.1%) and with the Organization for Economic Cooperation and Development average (28.4%) [35]. Thus, it is not enough that Korea should make efforts to lower the smoking rate at the governmental level. From this research, when genetic factors are controlled 100%, the men's occupations had the greatest influence on their smoking behavior, although socioeconomic factors did not have a major effect on stop-smoking behavior. For a more effective smoking-cessation policy, this should be kept in mind.
There are limitations to this research. First, the subjects who participated in the Korea Twin Study were limited to twins over 30 years of age and twins' family members over 20 years of age, so addressing smoking in teenagers was not possible. Second, in this research (based on a standard used to assess starting-smoking behavior), the standard for non-smokers was fixed at 400 cigarettes (lifetime), which was the information available for the existing cohort; this number is not based on existing research. Third, during the process of classifying the subjects according to occupation, given the number of people categorized as "others," such as housewives, students, unemployed, and retired, it was difficult to confirm all data for the head of a household, and, thus, we were unable to classify the subjects in a way that followed the occupation of the head of the household. Fourth, the information on smoking was based on data that the participants provided on the questionnaire; thus, no analysis using biochemical data was possible. Fifth, in terms of socioeconomic level, other than occupation, income, education level, residence, or parents'socioeconomic level or living style (rented house, house ownership, and monthly residence fee), a more detailed analysis was not possible. Sixth, this research is a cross-sectional study that observed socioeconomic levels and smoking behavior from the present point of view. Thus, a time-series assessment of how socioeconomic level caused the present situation was not available.
In conclusion, this research showed that even when genetic factors were 100% controlled, socioeconomic factors had a big effect on smoking. In terms of smoking cessation, genetic factors had a greater effect than environmental factors.
Notes
The authors have no conflicts of interest with the material presented in this paper.
This article is available at http://jpmph.org/.