Month and Season of Birth as a Risk Factor for Alzheimer’s Disease: A Nationwide Nested Case-control Study
Article information

Abstract
Objectives:
Season of birth, an exogenous indicator of early life environment, has been related to higher risk of adverse psychiatric outcomes but the findings for Alzheimer’s disease (AD) have been inconsistent. We investigated whether the month or season of birth are associated with AD.
Methods:
A nationwide nested case-control study including all community-dwellers with clinically verified AD diagnosed in 2005 to 2012 (n=70 719) and up to four age- sex- and region of residence-matched controls (n=282 862) residing in Finland. Associations between month and season of birth and AD were studied with conditional logistic regression.
Results:
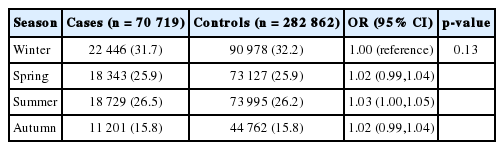
Month of birth was not associated with AD (p=0.09). No strong associations were observed with season (p=0.13), although in comparison to winter births (December-February) summer births (June-August) were associated with higher odds of AD (odds ratio, 1.03; 95% confidence interval, 1.00 to 1.05). However, the absolute difference in prevalence in winter births was only 0.5% (prevalence of those born in winter were 31.7% and 32.2% for cases and controls, respectively).
Conclusions:
Although our findings do not support the hypothesis that season of birth is related to AD/dementia risk, they do not invalidate the developmental origins of health and disease hypothesis in late-life cognition. It is possible that season does not adequately capture the early life circumstances, or that other (postnatal) risk factors such as lifestyle or socioeconomic factors overrule the impact of prenatal and perinatal factors.
INTRODUCTION
The importance of life-course perspective in dementia prevention has been acknowledged [1] and according to the Barker’s hypothesis, or the developmental origins of health and disease (DOHAD), the susceptibility to many chronic diseases is determined already in utero [2]. However, studies on the prenatal exposures and dementia face many practical challenges and are, to date, non-existent. Month or season of birth has been implied as an exogenous indicator of early life environment, i.e., a variable that is independent of individual circumstances at the time of birth and during the life course [3].
Season of birth has been suggested to increase the risk of adverse psychiatric [4] and neurological [5] outcomes. The findings have been most consistent for schizophrenia, with winter births being linked to higher risk of schizophrenia [4,6] and associated ventricular changes [7]. On the other hand, it has been suggested that the seasonal variation in schizophrenia has decreased, with evident seasonal association among those born in 1950s but no longer in those born in 1960s [8]. Studies on Alzheimer’s disease (AD) and dementia have been less consistent, with some studies reporting an excess of births in the first quarter of the year [9] or deficit of spring births [10] among AD cases and deficit of winter births among dementia cases [3]. Other studies have been unable to replicate this association [11-16]. This may be due to lack of power due to small sample size.
We investigated the association between month and season of birth in a nationwide nested case-control study (1:4, n=353 581) including all community-dwelling persons in Finland who received a clinically verified AD diagnosis in 2005 to 2011 (n=70 719).
METHODS
Study Population
The Medication and Alzheimer’s Disease cohort includes all community-dwelling persons of Finland, who received a clinically verified diagnosis of AD in 2005 to 2011 (n=70 719: AD cases of the present study). The age range was 34 to 105 years (mean, 80.1; standard deviation, 7.1 years) and 46 117 (65.2%) were females. In order to conduct a nested case-control study of the entire population of Finland, one to four age- matched (+/- one year), sex- matched and region of residence-matched controls were identified from the register that contains all residents of Finland who are entitled to benefits by the Social Insurance Institution (SII), i.e., all citizens and residents living in Finland for at least two years. The final study size was 353 581 (70 719 cases and 282 862 controls).
Each resident of Finland is assigned a unique personal identification code which was used link the participant data. All data were de-identified before submission to the research team and ethics committee approval or informed consent were not required as only de-identified data were used and the study participants were not contacted.
Diagnosis of Alzheimer’s Disease
AD cases were identified from the Finnish Special Reimbursement Register maintained by the SII of Finland as described in detail previously [17]. The Special Reimbursement Register contains records of all persons who are eligible for higher reimbursement due to certain chronic diseases, including AD. To be eligible for reimbursement, the disease must be diagnosed according to specific criterion and diagnosis statement must be submitted to the SII by a physician.
Briefly, the specific criterion for a clinically verified AD diagnosis are 1) symptoms consistent with mild or moderate AD, 2) a decrease in social capacity over a period of at least 3 months, 3) a computer tomography/magnetic resonance imaging scan, 4) exclusion of possible alternative diagnoses, and 5) confirmation of the diagnosis by a registered neurologist or geriatrician. The AD diagnosis was based on the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (now known as the Alzheimer’s Association) and Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria for Alzheimer’s diseases [18,19].
Exposures
Birth months were categorised to summer (June-August), autumn (September-October), winter (November-February) and spring (March-May).
Statistical Analyses
Statistical analyses were conducted with Stata version 12.0 (StataCorp, College Station, TX, USA). The association of exposures and AD were assessed with conditional logistic regression that accounted for matching. The p-values in Tables 1 and 2 represent the overall association between month or season of birth and AD (i.e., the p-value from conditional logistic regression model with AD as an outcome and month or season of birth as an exposure).

Association between month of birth and Alzheimer’s disease
Association between season of birth and Alzheimer’s disease
RESULTS
Birth months of the AD cases and controls are shown in Table 1. Month of birth was not associated with AD. There was some suggestion that AD cases were more commonly born in July than controls (odds ratio, 1.04; 95% confidence interval [CI], 1.00 to 1.08) but the absolute difference was only 0.3%. Similarly, no association was observed between season of birth and AD (Table 2), although there was some suggestion for winter births being less common, and summer births being more common among AD cases than in controls. However, the absolute differences were only 0.5% for winter births and 0.3% for summer births, respectively and the 95% CIs included 1.
DISCUSSION
We found no strong evidence that month or season of birth is related to risk of AD in our nationwide case-control study. There was some suggestion for lower prevalence of winter births among AD cases, but the absolute difference in those born during winter months between the cases and controls was very small. Thus, the results should be interpreted as null. Further, an adjustment for multiple comparison would render the p-values even further away from the conventional thresh-old of statistical significance.
Even though the inverse association between winter birth and AD was modest, our findings are in line with recent findings by Doblhammer et al. [3] who reported a deficit of winter births among dementia cases. They suggested that the association might be due to the thrifty phenotype and the developmental origins of health and disease hypotheses [2], or socioeconomic differences in the pro-creational habits, i.e., socioeconomic influences on seasonal conception/birth rates [3]. Previous studies that have assessed the association of season of birth and AD have often been based on small, selected cohorts which may impact their generalisability and make them unpowered to detect an association. The largest study to date included 727 AD cases [11], while three of the previous studies included less than hundred AD cases [14-16]. Similar to ours, majority of the previous studies concluded with null findings [11-16]. Thus, the two studies showing a seasonal effect [9,10] may be chance findings. Latitude/hemisphere is unlikely to explain the heterogeneity as the studies that found an association were conducted in Germany [3], UK [9], and Canada [10] while the null studies have been conducted in UK, US, Germany, Sweden and Australia [11-16]. Cohort effect, i.e., association dependent on year or decade of birth as shown for schizophrenia [8] does also not explain this heterogeneity.
One of the strengths of our study is the sample size. Thus, the null results are unlikely to be due to lack of power. We were able to identify all community-dwelling persons with clinically verified AD diagnosis. Further, due to the standardised diagnostic criteria, the positive predictive value of AD diagnosis in our study is high [20]. Some of the controls may have had undiagnosed AD, but it is unlikely that these undiagnosed cases would be unequally distributed across exposure categories, so this would dilute the estimates of our study towards the null by increasing the uncertainty around the point estimate. However, this would not affect the point estimate which was very close to 1 for all categories. Finland spans from the 60°N to 70°N and thus, the location of birth might matter. These data were not available, but the propensity for intermunicipal migration in Finland is rather low [19] and two-thirds of Finnish people live in the county where they were born [20]. Thus, especially in this age group, the location, or at least latitude, at the time of AD diagnosis was likely a very close approximation to their birth place. As our study sample was not selected on the basis of age, sex, socioeconomic position or e.g., participation in a certain insurance scheme, the findings should be fairly generalisable. Further, it is unlikely that ethnic background would affect the association between season of birth and AD/dementia. Thus the results should be generalisable also to other ethnic groups.
In conclusion, our nationwide study did not provide strong evidence that season of birth would affect the predisposition to AD. Although these findings do not support the hypothesis that season of birth is related to AD/dementia risk, they do not invalidate the DOHAD hypothesis in late-life cognition. It is possible that season does not adequately capture the early life circumstances, or that other (postnatal) risk factors such as lifestyle or socioeconomic factors overrule the impact of prenatal and perinatal factors.
Notes
CONFLICT OF INTEREST
Jari Tiihonen has served as a consultant to Lundbeck, Organon, Janssen-Cilag, Eli Lilly, AstraZeneca, F. Hoffman-La Roche, and Bristol-Myers Squibb. He has received fees for giving expert opinions to Bristol-Myers Squibb and GlaxoSmithKline, lecture fees from Janssen-Cilag, Bristol-Myers Squibb, Eli Lilly, Pfizer, Lundbeck, GlaxoSmithKline, AstraZeneca and Novartis; and grant from Stanley Foundation. Jari Tiihonen is a member of advisory board in AstraZeneca, Janssen-Cilag, and Otsuka. Marjaana Koponen has received personal research grant from Oy H. Lundbeck Ab foundation outside the submitted work. Other authors have no conflicts of interest associated with the material presented in this paper.