A Multi-level Analysis of Factors Affecting Participation in Health Screenings in Korea: A Focus on Household and Regional Factors
Article information

Abstract
Objectives
This study divided the factors that affect participation in health screenings into individual, household, and regional levels and conducted a multi-level analysis to identify the factors related to participation in health screenings.
Methods
Participants from the 2017 Community Health Survey were classified into 2 groups (under 40 and 40 or older). A multi-level logistic regression analysis was conducted to identify the factors that affected participation in health screenings.
Results
The screening rate of the participants was 69.7%, and it was higher among participants aged 40 and older (80.3%) than it was among participants younger than 40 (49.8%). At the individual level, the factors that influenced participation in health screenings included age, economic activity, smoking status, physician-diagnosed hypertension, and a moderate or high physical activity level. At the household level, the odds ratio of participation in health screenings was high for participants who lived in single-person households, lived with a spouse, earned a high monthly household income, and were not beneficiaries of national basic livelihood security. At the regional level, the odds ratio at the 95% confidence interval level of participation in health screenings was high for participants who had trust in the local community and lived in an area with a proportionally high social welfare budget.
Conclusions
This study analyzed nationalwide data and confirmed that individual, household, and regional characteristics affected participation in health screenings. Therefore, policies that prioritize the improvement of regional level factors and especially household level factors are likely to be the most effective for improving the screening rate.
INTRODUCTION
Health screenings are conducted to promote individual’s health through the early detection of cardiovascular diseases, such as hypertension and diabetes, and helping individuals obtain effective treatment and management [1]. Preventive treatment services through health screening can reduce future medical expenses [2], lead to simpler treatment options than if screenings are not conducted, and result in a good prognosis, ultimately guaranteeing the health of the general public. For these reasons, medical authorities strongly recommend receiving health screenings [3]. Despite the government’s efforts, the screening rate of the public dropped slightly from 78.5% in 2017 to 76.9% in 2018 [4].
Patterns in the utilization of medical services are influenced by individual characteristics as well as by the environmental factors that surround an individual [5]. An individual’s health is not just of concern to himself or herself alone, since it could also affect the individual’s family and friends as well as members of the local community. In this respect, diseases should be treated with the relationship between social and environmental factors in mind, in addition to individual characteristics such as health status and health behaviors [6]. However, previous studies that analyzed factors affecting health screening have focused mainly on individual characteristics, such as health-related behaviors [7–11].
According to a study that conducted a multi-level analysis to examine the factors that determined the screening rate for gastric cancer, hypothesized that the significant differences between regional variables could be better interpreted by conducting a multi-level analysis that incorporates more refined regional levels, such as the city, county, or district level, although the differences in cancer screening rates between regions could not be identified even when the regional level was set to the city/province level [12]. Another study that examined the factors related to cancer screening according to the marital status of Korean men and women, found the regional variable “non-apartment residency” to be significant. However, the number of regional samples was small, so while it was considered a meaningful variable, this finding is limited and further studies are needed [13]. Several studies in which single-level analyses were conducted on factors related to health screening participation determined that residential area significantly influenced individual participation in health screenings [9,14], and another found that the health screening rate varied between large and small cities and between urban and rural areas [15]. Studies that conducted multi-level analyses of health-related behaviors found that financial independence, the number of fast-food restaurants per 1000 residents, the crude divorce rate, the number of vehicle registrations, and the adjusted death rate had statistically significant effects on obesity [16], and that changes in the number of individuals with drinking problems could be explained by the number of pubs and changes in the crude divorce rate in areas where drinkers resided [17]. One study that found that the health screening rate of people with high community trust was greater than that of those with low community trust [18] also found that participation in health screenings cannot be attributed solely to individual characteristics. The study by Jeong et al. [19] that analyzed regional variables related to health level and health behaviors provides evidence in favor of establishing health policies tailored to the characteristics of specific regions. Previous studies that included a multi-level analysis of factors affecting participation in health screenings have mainly been related to cancer screening, and the regional level was usually set at the city/province level in those studies. Thus, there is a need for future studies that analyze the factors that affect participation in health screenings using both individual and household units, and at the city/county/district level.
This study conducted a multi-level analysis after classifying the factors that affect participation in health screenings into individual, household, and regional categories with the aim of providing basic data for developing policies to improve the screening rate, as well as identifying further factors related to participation in health screenings.
METHODS
Data and Participants
The 2017 Community Health Survey (CHS) was conducted among approximately 230 000 people under the direction of the Korea Disease Control and Prevention Agency (KDCA; formerly the Korea Centers for Disease Control and Prevention) with the aim of collecting health statistics at the city/county/district level in order to develop regional healthcare and medical plans, generate basic data to evaluate the performance of local healthcare projects, and establish a private-public cooperation system in local communities [20]. The participants in the present study were selected among those who answered “yes” or “no” to the question “Have you ever received health screening (excluding cancer screening)?” in the questionnaire from the 2017 CHS. According to the national health screening system, employee subscribers of National Health Insurance are eligible for general health screenings beginning at the age of 19, while dependents of employee subscribers and household members of subscribers are eligible for screening beginning at the age of 40. As such, the participants in this study were analyzed after being classified by age: under 40 and 40 or older.
Due to the limited number of previous studies that used a multi-level analysis to examine variables related to participation in health screenings, regional level variables were selected based on a literature review of studies that examined factors affecting participation in cancer screenings [12,13,21] and studies related to health behaviors [17,19,22–29]. Regional level variables were selected using the data from the 2017 CHS, and regional indicators for city/county/district units were taken from the Korean Statistical Information Service and the National Health Insurance Service (NHIS) website. First, we downloaded the raw 2017 CHS data from the KDCA website and matched regional indicators based on the public health center code. If the public health center code and a regional indicator did not match, the same regional indicators were collectively assigned to public health centers in self-governing districts based on the regional indicators. This choice reflected the assumption that the index values would be similar since public health centers within one self-governing district were located on adjacent streets and were subject to the same self-governing district policy.
Statistical Analysis
The 2017 CHS, which provided the data used in this study, collected multi-level data (hierarchical data) in which sample households were included in each sample region, and each individual was included in each sample household. Each of these groups was characterized by heterogeneity and dependency among individuals within the group [22]. Thus, a multi-level analysis was appropriate for overcoming ecological error.
The individual, household, and regional characteristics of the participants were confirmed using descriptive statistics. Differences in the screening rate by individual, household, and regional characteristics, as well as differences in the individual, household, and regional characteristics between groups of participants who did and did not participate in health screenings, were analyzed using the Rao-Scott chi-square test, given the complex sample design.
To determine the goodness-of-fit of the multi-level analysis, the intraclass correlation coefficient (ICC) was used to measure the presence of variability between each level. The ICC, which shows the percentage of the total variance between households and regions, can confirm the degree of household and regional variance among the total variance without inputting variables at each of the individual, household, and regional levels. A larger ICC suggests a higher explanatory power of household and regional characteristics affecting the dependent variable [30].
There were 4 possible research models for the multi-level analysis: (1) a model that included individual level variables alone, (2) a model that included individual level and household level variables, (3) a model that included individual level and regional level variables, and (4) a model that included all 3 variables. The explanatory power of each model could be obtained as the ratio of the variance of the research model to the variance of the null model. If the variance between households decreased when a household level variable was added at the household level, the added variable was deemed to have explanatory power for the difference in the health screening rate between households. Similarly, if the variance between regions decreased when a regional level variable was added, the added variable was deemed to have explanatory power for the difference in the health screening rate between regions. The proportional change in variance (PCV) caused by the added variable was calculated using the following equation.
Multi-level logistic regression analysis was performed to determine the correlation between variables at each level and health screening behaviors, and the results were presented as the odds ratio (OR) and 95% confidence interval (CI). SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for analysis, given the complex sample design of the CHS, and a generalized linear mixed model was applied using the PROC GLIMMIX procedure, which combines a generalized linear model and a linear mixed model for categorical data analysis of hierarchical data [31].
Ethics Statement
This study used raw data from the 2017 CHS. Since the data did not contain the participants’ personal information, a deliberation exemption was approved by the Institutional Review Board of Hanyang University (HYU-2020-05-019).
RESULTS
Screening Rates According to the Individual, Household, and Regional Characteristics of Participants
Table 1 shows the screening rates depending on the individual, household, and regional characteristics of the participants. The overall screening rate of the participants was 69.7%. The overall screening rates for those aged under 40 and those aged 40 or older were 49.8% and 80.3%, respectively.
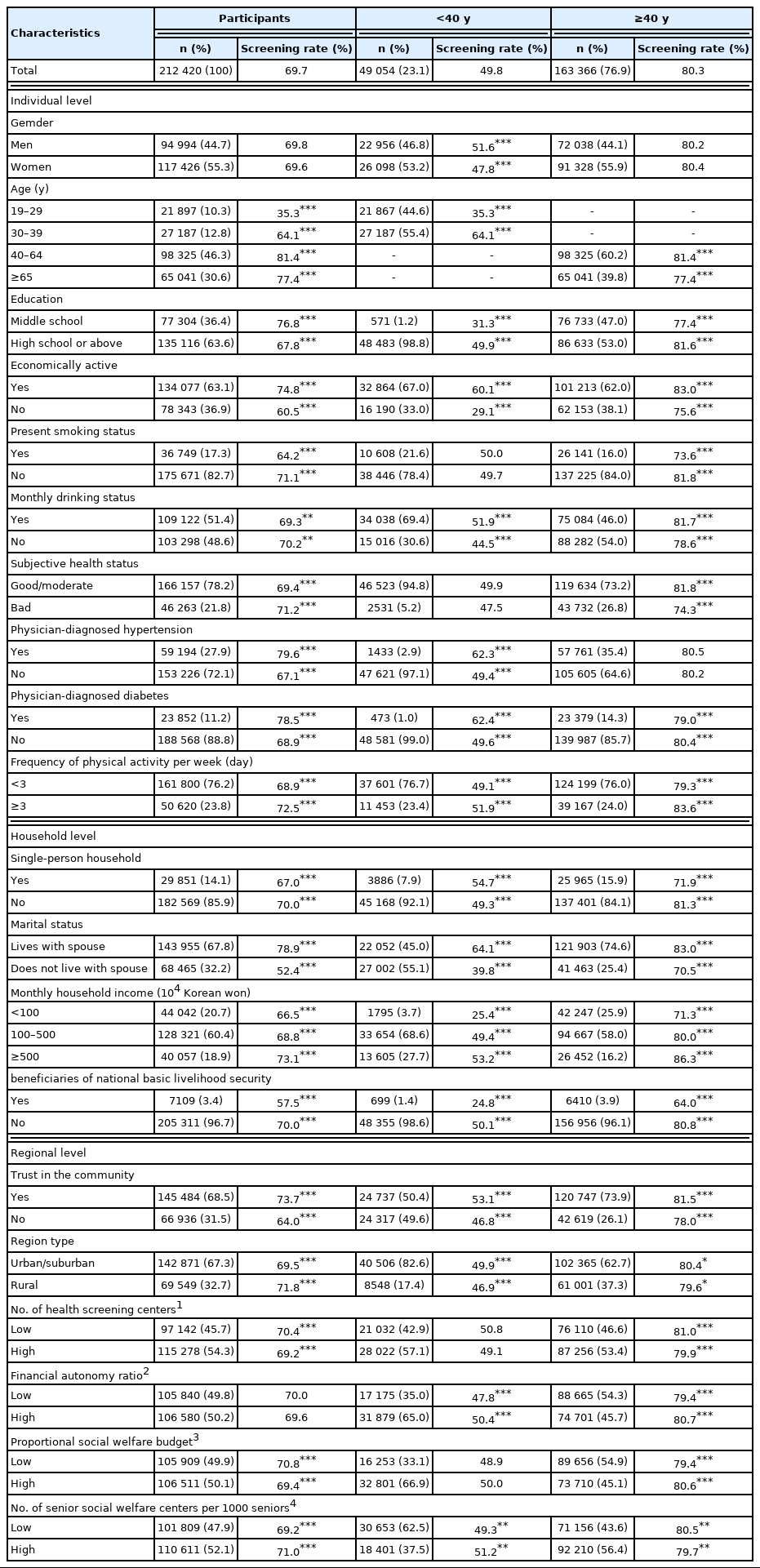
Screening rates according to participants’ individual, household, and regional characteristics
The screening rate for participants aged under 40 was high for participants who were men, aged 30–39, high school graduates or above, economically active, monthly drinkers, and previously diagnosed with hypertension or diabetes, as well as for those who lived with a spouse, had a high monthly household income, and were not beneficiaries of national basic livelihood security.
The screening rate for participants aged 40 or older was high for participants who were aged 40–64, high school graduates or above, economically active, non-smokers, monthly drinkers, and subjectively healthy, as well as when they engaged in moderate or high physical activity 3 days per week or more, lived in a multi-person household, lived with a spouse, had a high monthly household income, were not beneficiaries of national basic livelihood security, and had trust in their local communities.
Evaluation of Goodness-of- fit in the Multi-level Analysis
To determine the correlation between independent variables, Spearman’s correlation analysis was conducted between individual level variables, household level variables, and regional level variables. Among the regional variables that were selected based on previous studies, the number of doctors in medical institutions per 1000 people and the amount of green space per inhabitant were excluded because they were too similar to other variables included in this study—in particular, the number of health screening institutions per 10 000 people and whether participants lived in an urban or rural area. In the correlation analysis, the correlation (0.7) between the proportional social welfare budget and the number of senior social welfare centers was high. However, the multi-level analysis was conducted with a variance inflation factor (VIF) value of less than 10 in the multicollinearity analysis.
As shown in Table 2, the degree of variation between households (ICC) for the dependent variable was significantly low, ranging from 0.000 to 0.00038. This result suggests that the degree of change in the dependent variable had a significantly low explanatory power since the change according to the household level variable was 0.000–0.038% as opposed to the change according to the individual level variables. In cases when the ICC is less than 5%, a multi-level analysis is typically inappropriate due to the lack of homogeneity between the relevant factors [31]. However, if there is a theoretical basis, a multi-level analysis can be performed even in cases when the ICC is less than 5% [17,24]. This study conducted a multi-level analysis on a theoretical basis rather than a statistical basis since it aimed to determine whether household characteristics had an effect on participation in health screenings.

Evaluation of the goodness-of-fit of the multi-level analysis
Factors Affecting Participation in Health Screenings
Factors affecting participation in health screenings among participants aged under 40
Table 3 shows the results of the multi-level analysis of participation in health screenings by participants aged under 40. Model 4 concurrently analyzed the individual level, household level, and regional level variables. The OR of health screening participation was significantly high for participants who were men, aged 30–39, a high school graduate or above, economically active, not currently a smoker, a monthly drinker, and previously diagnosed with hypertension, as well as for those who engaged in moderate or high physical activity 3 days per week or more.

Factors affecting participation in health screenings
At the household level, the OR was significantly high for participants who lived in a single-person household, lived with their spouse, had a high monthly household income, and were not beneficiaries of national basic livelihood security.
At the regional level, the OR of participation in health screenings was significantly high for participants who had trust in the local community, resided in an urban area, lived in a region with a proportionally high social welfare budget (above the median), and lived in a region with a high number of senior social welfare centers per 1000 seniors.
Factors affecting participation in health screening among participants aged 40 or older
Table 3 shows the results of the multi-level analysis of participation in health screenings by participants aged 40 or older. Model 4 concurrently analyzed the individual, household, and regional variables. The OR of participation in health screenings was significantly high among participants who were women, 65 or older, economically active, and non-smokers, as well as those who had a good or moderate subjective health status, had been previously diagnosed with hypertension or diabetes, or engaged in moderate or high physical activity 3 days per week or more.
At the household level, the OR was significantly high for participants who lived in a single-person household, lived with their spouse, had a high monthly household income, and were not beneficiaries of national basic livelihood security.
At the regional level, the OR of participation in health screening was significantly high for participants who had trust in the local community and lived in a region with a proportionally high social welfare budget.
DISCUSSION
This study investigated the factors that affected participation in health screenings according to individual, household, and regional characteristics in order to raise the screening rate and further promote the health of the general public.
First, at the individual level, the factors related to participation in health screening among those under the age of 40 included gender, age, education level, economic activity, smoking status, monthly drinking status, previous hypertension diagnosis, and the degree of moderate-to-high physical activity, excluding subjective health status and previous diabetes diagnosis. Influential factors for those who were aged 40 or older included all of the variables except for education level and monthly drinking status. Previous studies have shown that, as the age of men increases, the screening rate also increases [9,30]. While this result was also found to be true among men under the age of 40, the OR of participation in health screening among women aged 40 or older was higher. All of the variables except for education level and monthly drinking status were found to have an influence on participants aged 40 and older. In addition, the screening rate decreased among those aged 65 or older. The screening rate of those engaged in economic activity was high. This is possibly due to the higher likelihood of employee subscribers to National Health Insurance, who are eligible for general health screening beginning at the age of 19, attending health screenings than those who are not employee subscribers. Nevertheless, the data in this study did not include information on the health insurance eligibility of the participants, and no firm conclusions can be drawn. However, under the assumption that eligibility for health insurance would affect participation in health screenings, this study categorized the participants into 2 groups: those under the age of 40 and those aged 40 or older. The OR (3.1) for participation in health screening was significantly higher for those aged 40 or older, as expected. A previous study also reported that the screening rate among seniors with good subjective health was high [14], and this study obtained similar results for those aged 40 or older. The results of previous studies that found that the screening rate among those with chronic diseases was high [7,19,25] were consistent with those of this study among the participants aged 40 or older who had been previously diagnosed with hypertension or diabetes.
Second, at the household level, there was a high likelihood of participation in health screenings among those who lived in single-person households, lived with a spouse, had a high monthly household income, and were not beneficiaries of national basic livelihood security. Previous studies have reported that the screening rate among those who lived in single-person households was lower than that of those who lived in multi-person households [26–28]. By contrast, in this study, the OR of participation in health screenings for single-person households was higher than that of multi-person households. In Park [28]’s study, many seniors who lived in single-person households were found to be widowed or divorced, and 17.3% of them were childless, whereas most of the individuals who lived in a multi-person household had spouses, and only 2.0% of them were childless, showed poor physical and psychological health, or a low level of human capital and economic status. The high screening rate of participants who lived in single-person households and were younger than 40 could be attributed to the need to participate in economic activity to maintain their lives as single people, and individuals who are employed likely have more opportunities to attend general health screenings or special screenings for their workplaces. Similarly, among the participants who were aged under 40, the screening rate of those aged 30–39 was higher than that of those aged 19–29. This result could also likely be attributed to economic activity, though further detailed investigations are needed to confirm these inferences. As monthly household income increased, the OR of participation in health screenings also increased, which is consistent with the findings of previous studies [9,26,27].
Third, among the regional level variables, trust in the local community and the proportional social welfare budget were determined to be factors affecting participation in health screenings for participants of all ages. For those under the age of 40, the number of senior social welfare centers per 1000 seniors in urban and rural areas was also determined to be a factor affecting participation in health screenings. At the regional level, the screening rate was high among those who had trust in their local communities, and there was no significant difference in the screening rate related to other variables. Social capital at the regional level implies trust in one’s community and neighbors, thus increases one’s sense of community. As a result, people with a strong sense of community more actively participate in health screenings, which suggests that individuals with positive views of their communities make more significant efforts to promote their own health [29]. The OR at the regional level was not higher than it was at the individual and household levels in this study, which was consistent with previous studies that found the influence of the regional level to be insignificant [17,18,32]. Lee and Kim [33] reported that the OR for the proportional social welfare budget, which was used as a regional level variable, was 0.991 (95% CI, 0.983 to 0.998), and it was 0.980 (95% CI, 0.970 to 0.996) in Kim[21]’s study. Because the ease of access to health screening institutions is proportional to the number of health screening institutions, the OR of health screening in urban areas was predicted to be high. However, this result was only significant for participants who were younger than 40. According to the results of additional analysis on the number of health screening institutions, the average number of health screening institutions per city/county/district in urban areas was 34, whereas it was 5 in rural areas. Nevertheless, the average number of health screening institutions per 10 000 people was 1.6 in urban areas and 1.4 in rural areas, showing no significant difference.
Fourth, the explanatory power at the household level and regional level was significantly lower than it was at the individual level. According to the ICC calculation results, which show the household level and regional level variance among the total variance of the model, the household level and regional level variance was determined to be 0.0002 and 0.0395, respectively, in the analysis of all participants. The household level and regional level variance was determined to be 0.02% and 3.95%, which was attributed to differences in households and regions. Typically, cases when the ICC is 5% or less are considered unsuitable for multi-level analysis [22] since it could prevent the influence of household level and regional level variables from being appropriately evaluated despite any significant results obtained regarding household level and regional level variables [28]. For this reason, some researchers believe that multi-level analysis is possible despite a low ICC when there is a theoretical basis for the study established by previous studies [30]. The small variance at the household and regional levels in this study resulted in a low explanatory power of household level and regional level variables regarding participation in health screenings. Despite this limitation, the results of this study suggest that the results at the household and regional levels obtained from the multi-level analysis are significant since previous studies have shown that household level and regional level variables are related to participation in health screening.
This cross-sectional study undertook a multi-level logistic regression analysis by utilizing 2017 CHS data, which did not show a temporal relationship between participation in health screening and major variables. In addition, the limitations of the data source prevented this study from being able to examine national health insurance eligibility, which has been found to have an effect on participation in health screenings and suggests the possibility of regional level variables being absent in the model despite the correlation of regional level data to participation in health screenings. Moreover, it was not possible to accurately match regional indicators to public health center codes since the CHS and regional indicators are generated by public health centers and local governments, respectively.
Nevertheless, this study used multi-level analysis to identify individual level, household level, and regional level factors that affect health screening behaviors, analyzed the influence of those factors, and undertook a multi-level analysis with three levels, which has not yet been covered in previous studies, to expand the scope of research on factors that affect participation in health screenings. This study examined the data based on public health centers at the city/county/district level, which is nearly identical to the basic breakdown of administrative units in Korea. Korea annually publishes Statistics Yearbook, which collects statistics on various variables such as population, education, and public health based on city/county/district level administrative units and facilitates understanding of these variables at different regional levels. It also further enables public health centers to utilize these data as basic data in the health promotion policy process for healthcare services that are suited to the characteristics of particular regions. In this regard, this study is significant in that it is the first study to analyze recent participation in health screenings among Koreans at the city/county/district level using the 2017 CHS data, which are representative of the national population.
This study found that the factors affecting participation in health screenings included the type of household in which individuals lived and the degree of trust individuals had in the local community, in addition to individual characteristics, such as gender, age, smoking status, and drinking status. This study also found that the influence of factors at the household level is stronger than that of factors at the regional level, which suggests that policies promoting psychological and economic stability within households would also lead to an improved screening rate. The influence of cohabitation with a spouse as a factor implies the significance of empathy, support, and care by others, which suggests that health policies should be established that provide psychological support and stability to individuals through community care services for those who cannot receive or receive limited family support due to divorce, bereavement, or separation. Furthermore, it is important to provide financial support to individuals so that they can recognize and maintain good health in addition to maintaining their everyday lives. It is already possible to identify beneficiaries of national basic livelihood security using local governments’ administrative systems, and beneficiaries should be further encouraged to participate in health screenings provided by the NHIS. Policies that can household level factors, as well as individual level and regional level factors, should be prioritized, as they would be the most effective at encouraging participation in health screening.
SUPPLEMENTAL MATERIALS
Korean version is available at https://doi.org/10.3961/jpmph.21.268.
ACKNOWLEDGEMENTS
None.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Both authors contributed equally to conceiving the study, analyzing the data, and writing this paper.