Well-being Index Scores and Subjective Health Status of Korean Healthcare Workers
Article information
 , Bohyun Park3,*, Nam-eun Kim4, Eun Jeong Choi5, Minsu Ock6, Sun Ha Jee7, Sue K. Park8, Hyeong Sik Ahn9, Hyesook Park4,5, Policy Development Committee of National Academy of Medicine of Korea (NAMOK)
, Bohyun Park3,*, Nam-eun Kim4, Eun Jeong Choi5, Minsu Ock6, Sun Ha Jee7, Sue K. Park8, Hyeong Sik Ahn9, Hyesook Park4,5, Policy Development Committee of National Academy of Medicine of Korea (NAMOK)Abstract
Objectives
The aim of this study was to evaluate the subjective level of health-related quality of life of Korean healthcare workers using various quality-of-life instruments.
Methods
This study included 992 participants, who were doctors and nurses. A survey was conducted between November 28 and December 4, 2019. Data from 954 participants divided into 3 groups (physicians, residents, and nurses) were analyzed. Four measurement tools (29 questions) were used in the survey to evaluate subjective health status and well-being.
Results
In the Mayo Well-being Index, burnout during work (88.5%) and emotional difficulties caused by work (84.0%) were frequently cited by the respondents. Regarding questions on burnout and emotional difficulties, residents and nurses had the highest scores (91.0 and 89.6%, respectively). Emotional problems, such as anxiety, depression, and irritability, accounted for a high percentage (73.1%) of the total, while 82.2% of respondents reported that their work schedules interfered with their leisure and family time. There was no significant difference among the groups in subjective health status. However, 10.1% of the residents experienced very low quality of life, which was a higher proportion than that of physicians (2.7%) and nurses (5.2%).
Conclusions
The level of well-being that Korean medical workers experienced in relation to work was lower than the results of the United States healthcare workers surveyed using the same tool. This study was unique in that it conducted a subjective quality-of-life survey on Korean healthcare workers.
INTRODUCTION
The health risks associated with medical institutions for patients are well-known [1], but there has been little interest in the health risks for healthcare workers. The demand for medical services has increased significantly, and legal and institutional regulations for the medical environment have been strengthened; this has led to overloaded and congested medical institutions [2].
Demands on healthcare workers, such as doctors and nurses, are expected to increase further, commensurate with the increased demand for medical services. To satisfy this increased demand, it is important to expand the number of healthcare personnel and to improve the productivity and quality of life (QoL) of existing personnel [3]. This is because healthcare workers can only provide high-quality medical services if they are in good health [4,5].
Rapidly changing aspects of the social and medical environments have had diverse and complex effects on the treatment and prognosis of patients, while also having potential negative impacts on the health, QoL, and well-being of healthcare workers. Although the well-being of healthcare workers is essential for high-quality patient care, data from the United States have demonstrated that clinicians experience high levels of burnout, with severe burnout reported by more than 50% of them [6].
Various programs have been developed in several countries to promote the health and well-being of clinicians and medical providers [7–9]. In order to manage the health of healthcare workers in Korea, it is necessary to establish a high-quality medical and therapeutic environment suitable for circumstances in Korea. The well-being of healthcare workers is important, considering that the physical, mental, and social health of medical staff can directly and indirectly affect patients. Qualitative research on health-related quality of life (HRQoL) perceptions has revealed a high incidence of work-related health problems among Korean healthcare workers [10].
The purpose of this study was to evaluate the subjective HRQoL among Korean healthcare workers using various quality-of-life instruments.
METHODS
Participants
In 2019, the number of healthcare workers in Korea was 537 952 (doctors: 127 258 and nurses: 410 694), and about 0.2% of the potential population participated in the study [11]. An online survey of 1000 people, including 400 physicians, 300 residents, and 300 nurses, was conducted between November 28 and December 4, 2019. Among these people, 992 who understood the purpose of the survey and volunteered to participate were enrolled in this study; 954 were included in the final analysis, after excluding 38 who did not complete the survey or answered it incorrectly. The participants who identified themselves as doctors (trainees) in the survey questionnaire were classified as residents, those who responded that they were doctors (medical specialist) were categorized as physicians, and the others were classified as nurses.
Online Survey Method
To evaluate the subjective health and well-being of healthcare workers, questions were asked via the online platform SurveyMonkey. The questionnaire was sent to the National Academy of Medicine of Korea, Korea Public Health Association, Korean Medical Association, Korean Intern Resident Association, and university hospitals, and to healthcare workers via e-mail and text messages. The completed questionnaires were collected through SurveyMonkey until the target number of subjects was reached.
Study Measures
Four questionnaires were used: the Mayo Well-being Index (WBI), which was specifically developed for healthcare workers in the United States, and the Korean versions of the EuroQol 5-Dimension 5-Level (EQ-5D-5L), the Health-related Quality of Life Instrument with 8 Items (HINT-8), and the EuroQol visual analogue scale (EQ-VAS). These instruments (EQ-5D-5L, HINT-8, EQ-VAS) are used to evaluate subjective health status and well-being in the general population. The questionnaire used in this study consisted of a total of 23 questions about well-being from the WBI (9 questions), EQ-5D-5L (8 questions), HINT-8 (5 questions), and EQ-VAS (1 question), and 6 questions about basic information.
Well-being Index
The Mayo WBI questionnaire [12] includes 9 standardized items pertaining to aspects of QoL, including burnout, mental and physical QoL, depression, fatigue, and stress. Approval was obtained from the Mayo WBI development team for the use of the Korean version of this instrument. The research team translated the questions into Korean under the supervision of the National Institute of the Korean Language, and then commissioned a language review company to perform a reverse translation. The survey was conducted after receiving final approval from the Mayo Clinic for the use of the Korean version of the WBI. Questions 8 and 9 were scored using a Likert scale ranging from −2 (low risk) to 9 (high risk).
EQ-5D-5L
The EQ-5D-5L [13,14] is a QoL assessment tool developed by the EuroQoL group in Europe, covering 5 areas: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In the EQ-5D-5L, a health status profile is derived based on the scores in each domain. The results were converted using the value set developed for Korea in 2016 [15]. The converted scores ranged between −1 (highest risk) and 1 (lowest risk).
HINT-8
The HINT-8 (Korean version) [16] is a measurement tool developed by the Korea Centers for Disease Control and Prevention for use in the Korea National Health and Nutrition Survey. It was designed to measure HRQoL in Koreans.
EQ-VAS
The EQ-VAS is used to quantitatively assess health status. Respondents select a number between 0 (worst health imaginable) and 100 (best health imaginable) to represent their health status [17].
Statistical Analysis
Data analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics were generated to summarize the general characteristics of the participants. For categorical data, the groups were compared using the chi-square test. The Fisher exact test was performed when there were <5 observed values. To assess the subjective health status and QoL of healthcare workers, a general linear model was used, with adjustment for sex and age. Results are presented as adjusted means and 95% confidence intervals. A two-tailed p-value <0.05 was taken to indicate statistical significance.
Ethics Statement
This study was approved by the Institutional Review Board of Ewha Womans University (No. EUMC-2019-10-032).
RESULTS
Table 1 shows the distribution of participants by sex, age, and occupation. In total, 954 subjects were analyzed; the female to male ratio was 1.8 (n=614 and 340, respectively). There were 369 physicians (38.3%), 307 nurses (32.2%), and 278 residents (29.1%). Among the nurses, there were 6 males and 301 females (98.0%). The largest age group was 30–39 years in the overall sample and 20–29 years among nurses. On average, the physicians were older than the residents and nurses. In total, 44 physicians (11.9%) were aged ≥60 years, while no residents and 1 nurse (0.3%) belonged to that age group.

Demographic characteristics of the study participants
According to the results for the Mayo WBI (Table 2), 844 (88.5%) respondents felt burned out while working in the past month, while 801 (84.0%) had experienced emotional difficulties due to work. Thus, most of the respondents reported negative physical and mental experiences related to their jobs. The rates of burnout and emotional difficulties were highest among residents, followed by nurses (91.0 and 89.6%, respectively). Most subjects (73.1%) reported emotional problems, such as anxiety, depression, or irritability, while 58.4% (n=557) stated that their physical health had interfered with their daily life and work (especially the residents; n=185, 66.6%). However, 93.4% of the respondents reported that they felt that their work was meaningful. Regarding the final survey item, (pertaining to whether or not the work schedule interfered with leisure or family time (answered on a 5-point scale), 82.2% of the respondents reported some level of interference.
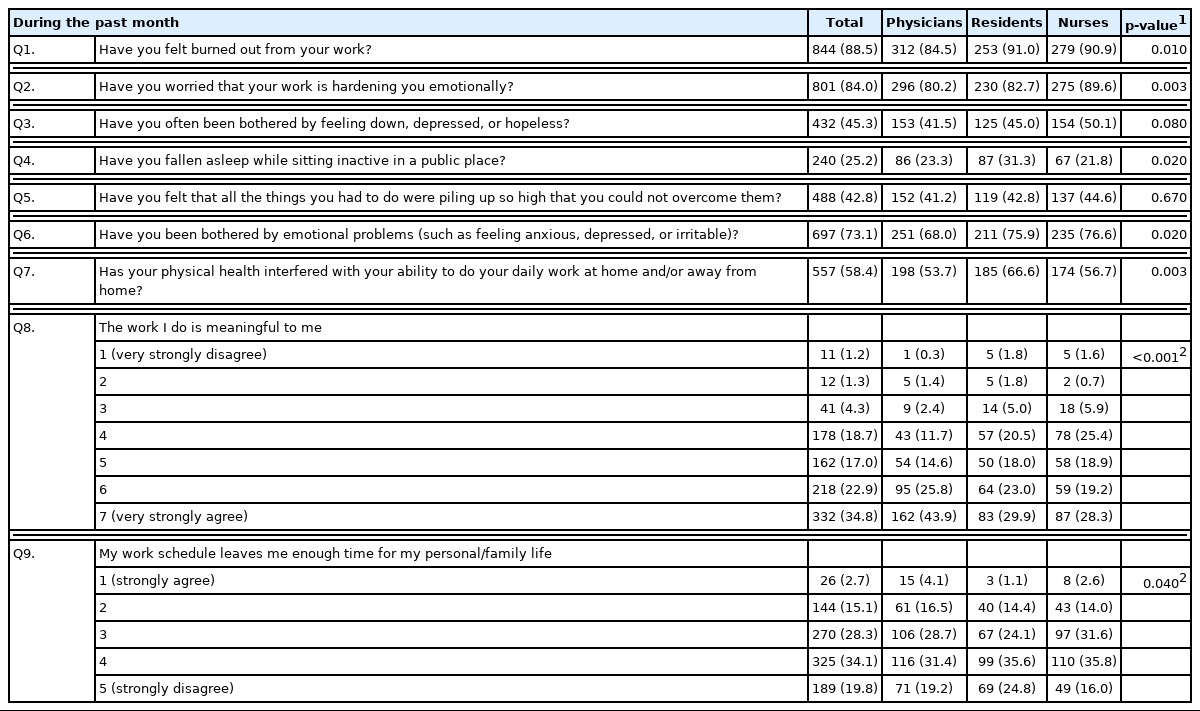
Well-being Index results of healthcare workers in Korea
Table 3 shows the differences in subjective QoL among the physician, resident, and nurse groups. Mayo WBI scale scores range from −2 to 9, with higher scores representing a lower QoL. The mean±standard deviation (SD) WBI score was similar among the groups (4.0±2.5) after adjustment for sex and age. The EQ-5D-5L and HINT-8 scores range from 0 to 1, with scores closer to 1 representing a higher QoL. The mean EQ-5D-5L score was 0.85±0.09, while the mean HINT-8 score was 0.78±0.08. The EQ-VAS scores range from 0 to 100 (best health imaginable). The mean EQ-VAS score was 71.5±18.2. The subjects in the 20–29 years age group had the lowest EQ-VAS scores (66.1±19.2), and the scores for subjective health conditions were higher in those aged ≥30 years.

The WBI scores of the physician, resident and nurse groups are shown in Table 4. Residents had the highest frequency of WBI scores >8 among the 3 groups, and 10.1% of the residents experienced a very low QoL; this was a higher proportion than observed in the physician (2.7%) and nurse (5.2%) groups.
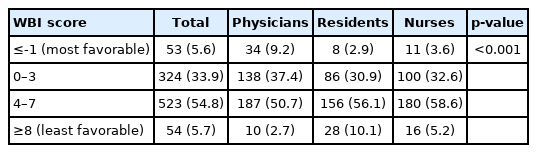
Well-being Index (WBI) scores of Korean healthcare workers by occupational group
DISCUSSION
In our survey of 954 medical professionals, 88.5% of the doctors and 84.0% of the nurses reported that they experienced burnout (Mayo-Q1) or emotional difficulties (Mayo-Q2) due to their job. More than 58% of the respondents reported that physical health problems interfered with their work and daily lives (Mayo-Q7). The mean WBI was 4.0, and the reported well-being was lower among Korean healthcare workers than has been reported among healthcare workers in other countries.
A comparison of the subjective QoL of our Korean respondents with a United States sample from a 2013 study (1667 participants) [18] demonstrated that the former group had higher frequencies of “yes” responses for Mayo-Q1, Mayo-Q2 (job-related emotional difficulties), Mayo-Q4 (sleeping in public places), and Mayo-Q6 (emotional problems, such as anxiety, depression, and irritability) scores, by 29.8% (70.1 vs. 91.0), 44.8% (57.1 vs. 82.7), 40.4% (22.3 vs. 31.3), and 17.3% (64.7 vs. 75.9). Frequent feelings of depression or despair (Mayo-Q3) were reported by 44.1% and 45.0% of the United States and Korean respondents, respectively. Stress caused by a heavy workload was higher in the United States sample (54.2%) than in the Korean sample (42.8%), while 25.1% of the United States sample and 66.6% of our Korean respondents reported that their physical health interfered with their daily lives and work. Physical fatigue levels were more than twice as high in the Korean group than in the United States group. Overall, the subjective QoL of the former group was significantly lower than that of the latter.
In a 2018 survey of 1576 United States nurses (National Sample Survey) [19], the mean WBI scores of female nurses and physician assistants were 0.7±2.4 and 0.77±2.47, respectively. The mean score for male nurses (0.49±2.30) was lower than that for female nurses, reflecting higher well-being; more than 60% of the participants had a score below 1.0. In this study, the mean WBI score for 307 nurses was 4.20±2.28, which was 5 times higher than reported in the United States sample. In addition, the well-being level of the Korean healthcare workers was more than 3 times higher in all WBI categories (burnout, depression, anxiety, stress, fatigue, and QoL).
The Mayo WBI data showed that the level of well-being of our Korean healthcare workers was lower than that of workers in other countries. Some countries have developed programs to improve and maintain the well-being of healthcare workers. The National Academy of Medicine (Rochester, MN, USA) developed a program promoting doctors’ well-being in 2007 evaluating all factors affecting the well-being, satisfaction, and productivity of doctors [20]. The National Academy of Medicine is working with a network of 60 organizations on the “Clinician Well-Being and Resilience” program to discuss and share action plans to promote the well-being of clinicians nationwide, and improve clinical well-being at the individual and system level [21]. The Mayo Clinic, National Academy of Medicine, Canadian Medical Association [22], and Australia Health Practitioner Regulation Agency [23] conduct surveys of medical personnel to improve healthcare systems and the welfare of healthcare workers.
The Korean Medical Association conducted the first national survey of healthcare workers’ well-being in 2016 [24], with a second survey conducted in 2020. These large-scale surveys of all doctors in Korea identified various problems in the work environment. They provided important evidence for policy development [25]. The Korea Nursing Health Research Cohort study has been conducting surveys every 6 months to determine the health and occupational problems, and risk factors thereof, of nurses [26]. However, surveys on QoL are lacking. Customized health research programs using surveys developed for healthcare personnel are needed in Korea.
Compared to a 2017 survey of the general Korean population using the HINT-8 and EQ-5D-5L [27], the HRQoL of our healthcare workers was lower in all domains. In particular, there were fewer positive responses on the EQ-5D-5L pertaining to pain/inconvenience and anxiety/depression in the general population (18.6 and 21.9%, respectively) than among our healthcare workers (61.7 and 65.6%, respectively). In other words, the physical and mental QoL of the healthcare workers was more than 3 times lower than that of the general population. The HINT-8 results also reflected lower HRQoL among our healthcare personnel than among the general population, on all 8 survey items. Considering that the mean age of our participants was 37.4 years (8 years younger than that in the 2017 study [45.5 years]), it appears that the development and implementation of healthcare interventions should be prioritized for healthcare workers in Korea.
Although the representativeness of this study was limited by the Internet-based recruitment method, it was nevertheless significant in that it assessed the subjective QoL of healthcare workers in Korea using instruments specifically developed for that population. This study used members registered as clinical healthcare personnel in the association as sample groups among all doctors and nurses. The number of people in the sample group is expected to be smaller than that of the population, but there was a limitation in accurately estimating the response rate because it was difficult to obtain information on the sample group due to reasons related to the protection of personal information. The well-being of doctors and nurses has a significant impact on their rapport with patients. Studies have established that increased trust between healthcare workers and patients improves treatment compliance and effectiveness [28–30]. In the future, it will be necessary to evaluate the QoL of Korean healthcare workers through surveys using representative sampling methods. National well-being programs for healthcare workers could enhance the overall productivity and satisfaction of this group, ultimately improving the quality of patient care.
CONCLUSION
The emphasis on the concept of service in healthcare has led to an increase in patients’ demands and difficulties in maintaining the well-being of individuals in busy and crowded hospital settings. This study conducted a subjective QoL survey among Korean healthcare workers, and some results showed low QoL scores. Healthcare workers are often exhausted for a variety of reasons, which has a negative impact on patient care. Long-term institutional improvements and research are needed to improve the clinical environment at the social level. Based on this survey, the factors that improve well-being must be considered in policy-making. More research on job-related risk factors for poor health is also necessary.
ACKNOWLEDGEMENTS
None.
Notes
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
FUNDING
This research was supported by a grant of the National Academy of Medicine of Korea (2019).
AUTHOR CONTRIBUTIONS
Conceptualization: Jee SH, Park SK, Ahn HS, Park H. Data curation: Shin Y, Park B, Kim NE, Choi EJ, Ock M. Formal analysis: Shin Y, Park B. Funding acquisition: Park H. Methodology: Shin Y, Park B, Ock M. Project administration: Ock M, Jee SH, Park SK. Visualization: Shin Y, Park B. Writing – original draft: Shin Y, Park B, Kim NE, Choi EJ. Writing – review & editing: Ock M, Jee SH, Park SK, Ahn HS, Park H.