
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 45(4); 2012 > Article
-
Original Article
Health Impact Assessment of Free Immunization Program in Jinju City, Korea - Keon Yeop Kim1, So Youn Jeon2, Man Joong Jeon3, Kwon Ho Lee4, Sok Goo Lee5, Dongjin Kim6, Eunjeong Kang7, Sang Geun Bae1, Jinhee Kim8
-
Journal of Preventive Medicine and Public Health 2012;45(4):267-275.
DOI: https://doi.org/10.3961/jpmph.2012.45.4.267
Published online: July 31, 2012
1Department of Preventive Medicine, Kyungpook National University School of Medicine, Daegu, Korea.
2Department of Emergency Medical Technology, Daejeon Health Sciences College, Daejeon, Korea.
3Department of Preventive Medicine and Public Health, Yeungnam University College of Medicine, Daegu, Korea.
4Department of Satellite Geoinformatic Engineering, Kyungil University, Gyeongsan, Korea.
5Department of Preventive Medicine, Chungnam National University School of Medicine, Daejeon, Korea.
6Division for Health Promotion Research, Korea Institute for Health and Social Affairs, Seoul, Korea.
7Department of Health Administration and Management, Soonchunhyang University, Asan, Korea.
8Institute of Health Science, Korea University College of Health Science, Seoul, Korea.
- Corresponding author: So Youn Jeon, DrPH. 21 Chungjeong-ro, Dong-gu, Daejeon 300-711, Korea. Tel: +82-42-670-9413, Fax: +82-42-670-9584, jsy0416@hit.ac.kr
Copyright © 2012 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- This study was conducted to assess the potential health impacts and improve the quality of the free immunization program in Jinju City by maximizing the predicted positive health gains and minimizing the negative health risks.
-
Methods
- A steering committee was established in September 2010 to carry out the health impact assessment (HIA) and began the screening and scoping stages. In the appraisal stage, analysis of secondary data, a literature review, case studies, geographic information systems analysis, a questionnaire, and expert consultations were used. The results of the data collection and analyses were discussed during a workshop, after which recommendations were finalized in a written report.
-
Results
- Increased access to immunization, comprehensive services provided by physicians, the strengthened role of the public health center in increasing immunization rates and services, and the ripple effect to other neighboring communities were identified as potential positive impacts. On the other hand, the program might be inaccessible to rural regions with no private clinics where there are more at-risk children, vaccine management and quality control at the clinics may be poor, and vaccines may be misused. Recommendations to maximize health gains and minimize risks were separately developed for the public health center and private clinics.
-
Conclusions
- The HIA provided an opportunity for stakeholders to comprehensively overview the potential positive and negative impacts of the program before it was implemented. An HIA is a powerful tool that should be used when developing and implementing diverse health-related policies and programs in the community.
- As the most cost-effective health service [1-3], immunization for children has significantly decreased the incidence of measles, mumps, rubella, polio, diphtheria, pertussis, and tetanus [3]. Since the introduction of inoculation in 1882, Korea has emphasized and expanded its immunization program to fund and provide childhood immunization services through public health centers [4]. However, this program has geographical and economic barriers, because it is only available at public health centers and not at private clinics [5]. In order to improve access to childhood immunization, the Korean government launched the National Immunization Program in March 2009, in which the government supports 30% of the cost of vaccines received at private clinics. However, the program still imposes an economic burden on the public for receiving vaccinations [6].
- In June 2009, Gangnam-gu, one of the 25 sub-districts of Seoul Metropolitan City, was the first to offer free immunization at clinics. This scheme has now spread to many other local governments. In reaction to this trend, Jinju City launched the Jinju Free Childhood Immunization Program in January 2011. Children in Jinju can now receive free vaccinations from private clinics. The goal of the program is to improve the health of children living in Jinju by creating a supportive environment for those who experience geographic and economic difficulties in accessing vaccinations. Children under 12 years can receive the 8 vaccines in the national immunization schedule for free, which includes a total of 22 visits (BCG, hepatitis B, DTaP, polio, MMR, Japanese encephalitis, varicella, and Td).
- A health impact assessment (HIA) is a method of analyzing the impact of a project on its subject in terms of public health. It is a combination of processes, methods, and means to determine the potential impact and the distribution of impacts of health from a policy, program, or project within the target population. HIAs aim to modify the proposed policy to minimize the negative impact and maximize the positive impact by improving the knowledge of the potential impact of a policy or a program and announcing them to the decision makers and the target population [7]. HIAs have been used in addressing various determinants of health including urban planning, agriculture, environment, culture, energy, housing, welfare, and transportation [8]. HIA papers published in Korea are mostly retrospective HIAs on environmental diseases [9], and papers introducing the concept of HIA [10,11]. HIAs on welfare, such as one on the Dream-Start Center, and on urban planning, such as one on local government-led park development, have recently been published, widening the range of HIA in Korea [9,12].
- This study scientifically analyzes the health impacts of the Jinju Free Childhood Immunization Program in participation with stakeholders in order to suggest recommendations that maximize the positive impacts and minimize the negative impacts of the program.
INTRODUCTION
- The HIA of the Jinju Free Childhood Immunization Program was conducted from September to November 2010 according to the HIA guidelines developed by the World Health Organization [8], the Merseyside guidelines [13], and the Korea Institute for Health and Social Affairs [14]. The procedure used is illustrated in Figure 1.
- An HIA can include various steps depending on the researchers or institutions, but typically consists of screening, scoping, appraisal, reporting, implementation, and evaluation [10,13,15,16]. For our study, a steering committee was formed as the main decision-making body, conducted the screening process, and determined the scope of the study. After understanding the background and the overall plan of the program, secondary data on the demographics (especially on the vulnerable population), health care institutions delivering immunization services, number of vaccinations and rates of enrollment in the electronic registration system, and the incidence of infectious diseases were collected.
- In the appraisal stage, which determines the potential positive and negative health impacts, a literature review, case studies, geographic information systems (GIS)-assisted analysis of the immunization service coverage area, and a community survey were conducted. Advisory meetings were held with experts, immunization service staff at the Korean Centers for Diseases Control and Prevention and public health centers in other regions who already were implementing this program. A series of workshops were held with community representatives, doctors, and government officers to discuss the results of the collected data and consultations and recommendations were developed.
- Steering Committee Organization
- The steering committee of the Jinju Free Childhood Immunization Program consulted with each other in stages throughout the project, including screening, scoping, and appraisal, and attended workshops for developing recommendations for suggesting program alternatives. The steering committee consisted of 9 members from the local area: 2 pediatric physicians, 1 representative from a women's non-governmental organization, 1 from a childcare facility, 1 mother, 1 HIA expert, 1 local professor from a college of medicine, 1 public health center immunization staff person, and 1 public health center HIA staff person.
- Screening
- Screening is the process of determining whether the policy or project is suitable and necessary for an HIA. In our study, the steering committee modified the guidelines developed by New South Wales, Australia, [17] to decide whether the Jinju Free Childhood Immunization Program needed to undergo an HIA. As a result of screening, the steering committee decided to undertake an HIA.
- Scoping
- In the scoping stage, the procedure and the scope of the assessment was planned. In this stage, the type of assessment to undertake is determined by the available time and resources. The steering committee at Jinju decided to perform a rapid assessment, which would require relatively little time and few resources.
- Appraisal
- The secondary data analysis, literature review, case studies, community surveys, GIS-assisted analysis, and consultation with experts were determined as the appraisal methods through the scoping process. The coverage population, infectious disease incidence, and immunized population were identified through secondary data analysis. A literature review on immunization programs and case studies of other regions that have implemented fully funded immunization programs were conducted. A community survey was conducted with local representatives, welfare facilities representatives, residents, and members of women's organizations. A total of 31 people answered the survey. The GIS-assisted analysis examined graphically the expected increase in the coverage area resulting from the free immunization service. Although the coverage area is difficult to define due to the factors of clinics, geographical conditions, population distribution, traffic conditions, and influence of other nearby medical institutions [18], we mapped the coverage area by distance, considering that the free immunization service is a primary health service for children. The coverage area was mapped by 250 m, 500 m, and 1000 m distances from the clinics based on the typical walking distance of children. The distribution of the immunization target population and private clinics in 2009 was also reviewed. Experts were consulted, workshops were held, and policy recommendations were derived.
METHODS
- Immunization Status of Children in Jinju
- As of 2010, there were a total of 45 520 children (12 years of age or younger) who comprised the target population for immunization services. An average of 576 children lived in the eop and myun areas and an average of 1729 children lived in the dong areas. Most of the subjects lived in the dong areas. Children in the vulnerable group included 702 children in multicultural families, 17 children with dependents, and 9704 children in the child welfare system.
- As for the clinics offering immunization services, most were concentrated in the downtown regions of the dong areas. In the dong areas, and myun areas near dong areas, private medical clinics were responsible for immunizations, while public health centers covered the eop and myun areas (Figure 2).
- The estimated immunization rate for BCG, DTaP 1, 2, and 3, polio 1, 2, and 3, and MMR 1 and varicella was high for children under 24 months old, but lower for later booster injections (Table 1).
- With the exception of mumps and varicella, there was almost no incidence of vaccine preventable diseases in 2009. The incidence rate in Jinju was 30.49 per 10 000 population members, which was lower than the national occurrence of 137.24 people for every 10 000 people.
- Case Studies
- Case studies at other local governments that implemented the Free Childhood Immunization Program prior to Jinju were reviewed. The Korean Centers for Disease Control and Prevention implemented the Expanded National Immunization Pilot Program in Gunpo and Daegu in 2005. In Gunpo, the program yielded an increased participation and share of medical clinics, improved accessibility due to shorter travel time, increased initial DTaP immunization rate, and improved overall children health services [19]. In Daegu, the program yielded high immunization rates of BCG, DTaP 1 and 2, and IPV 1 and 2 [20]. In Gangnam-gu, Seoul, where the first fully-funded immunization services in the nation were implemented in June 2009, quantitative and qualitative improvement of the vaccination services in comparison with adjacent districts was observed [21].
- Community Survey Results
- The opinions collected from a survey of members of the steering committee who were local residents or representatives of welfare facilities or women's groups are as follows. The positive qualities of the program were time savings from increased accessibility to service providers and cost reduction. Other positive impacts included the availability of private clinics when public health centers are closed, the possibility of medical examinations for infants and checking health status along with the vaccinations, and the provision of the service by the primary care doctor leading to reduced risk and readily available follow-up treatment. Negative impacts that were identified included the possibility of increased taxes or a reduced budget for other projects and the management and supervision of the vaccines. Other negative perceptions included over-charging for the vaccines, overuse of the vaccines, and the increased number of patients going to private medical institutions. Other suggestions included hope for expanded free immunization and announcement of the immunization schedule and of missed immunizations by computerized enrollment.
- Geographic Information Systems-assisted Analysis
- Figure 3 illustrates the free immunization service coverage area from public health centers in the downtown areas in a 250 m to 1 km radius (service area within walking distance). When private clinics are included, the coverage area increases significantly and includes most of the downtown area. Also, about 80% of the target population lives within the service areas of private clinics, as of 2009, and the program is expected to dramatically improve the accessibility to citizens (Figure 4).
- Health Impacts
- The potential positive and negative health impacts of the Free Childhood Immunization Program derived from the steering committee meetings and workshops and advisory meetings are listed in Table 2.
- First, improved access to immunization services is expected as private medical institutions will be offering the service. GIS analysis results show that most of the target population lives within the service areas of private clinics, which will significantly improve accessibility. Second, the immunization rates will increase. Enrollment in the electronic immunization registration system will increase with the active participation of private clinics, which, in turn, will decrease the incidents of duplicated vaccination cases. Third, health and medical services are offered holistically by the primary care provider at private clinics. This will decrease revisits to health care institutions and reduce time and travel costs. Fourth, the public health center can take a coordinating role and concentrate on improving the overall local immunization services. Fifth, the program can be a good countermeasure to the low birth rate in Jinju. Jinju is becoming a city with aging population issues, including low birth rates, but compared to its counterparts, it lacks countermeasures. Sixth, the program is expected to be expanded to other local governments in the vicinity, which will contribute to overall improvement of child vaccination in Gyeongsangnam-do.
- Although there are no apparent negative health impacts from the implementation of the Free Childhood Immunization Program, the following issues should be considered. First, although this project improves accessibility, most of the private clinics are located in the downtown area and will have little or no impact in rural areas, where most of the vulnerable population resides. Second, vaccine management could be inadequate. Currently, public health centers maintain the cold-chain with specialized vaccine refrigerators, are prepared for blackouts, other emergencies, and expiration dates, and these measures are usually better implemented than they are in private clinics. Third, a problem could arise from the quality of the vaccination staff. Although doctors conduct immunizations in most private clinics, sometimes staff with inadequate medical knowledge and skills can inject vaccinations. In the case of public health centers, vaccination staff receives training according to a regular schedule. Fourth, private clinics may use more expensive vaccines, and might burden citizens economically.
RESULTS
Immunization target population and clinics offering immunization services
Immunization rate
Incidence of infectious diseases
Positive health impacts
Negative health impacts
- The main purpose of an HIA is to increase knowledge of the potential impacts of a policy, minimize the negative impacts, maximize the positive impacts, and lead the proposed the policy in a more health-friendly direction. To do so, this study collected the opinions of various stakeholders before implementing the Jinju Free Childhood Immunization Program and reviewed the possible positive and negative impacts on health. This section aims to review the recommendations in implementing the Jinju Free Childhood Immunization Program and discusses the methods of the HIA.
- Recommendations for the Jinju Free Childhood Immunization Program
- The recommendations for increasing the positive impacts and decreasing the negative impacts of the program are as follows (Table 2). Local public health centers should take the following into account. First, since the direct practice of vaccination is being transferred to private clinics, public health centers should concentrate on management of the immunization program. Health centers should provide the private clinics with vaccine management and vaccination manuals and self-checklists, as well as manage and supervise the whole program. In addition, public health centers should continue to provide education programs for the vaccination staff in cooperation with the local physicians' organization. Second, public health centers need a strategy for increasing the rates of vaccine booster injection administration for infants older than 2 years old. Third, the local government should develop alternative plans for areas where the accessibility to immunization is not improved, as well as a detailed plan to improve the immunization rate of the vulnerable class of the population. Fourth, the local government must actively advertise the program so that the entire population (especially the vulnerable class) can benefit from it. Fifth, the local government should not decrease resources for other welfare programs as a result of implementing this program. Sixth, the local government should ultimately consider providing full support for elective vaccinations (pneumococcal, rotavirus, etc.). In this case, children in the vulnerable population, who live in group facilities, should take the highest priority. Seventh, the local government must develop a system to monitor and evaluate the free immunization program. Eighth, a partnership framework in the local community needs to be developed. Cooperation with doctors and local child centers where the children of the vulnerable class usually reside, the Department of Social Welfare, and the Department of Education is necessary.
- Private clinics should consider the following. First, private clinics should manage the quality of vaccine storage and education of vaccination staff. The local physicians' organization should cooperate with the public health center in developing strategies for management and advertisement of the program. Second, smaller private clinics may face potential problems in the supply of vaccines. These clinics should especially be prepared for a sudden increase in patients during the initial stages of the program. Third, private clinics should provide medical examinations for infants in addition to vaccinations. Once the responsibility of vaccination is transferred to private clinics, a plan to transfer the responsibility of medical examinations for infants is needed. Fourth, for elective vaccinations and other vaccinations which are not part of the mandatory immunization list, a detailed explanation should be given to the parents to eliminate distrust of physician-induced demand.
- Issues Involving the Methods of Health Impact Assessment
- Generally, studies on vaccinations in Korea have focused on the factors that influence the immunization rates [22-24] and results from pilot programs [19-21]. In contrast, the Jinju HIA reviewed possible positive and negative impacts of the policy with various stakeholders, and recommended modifications to the plan. This process provided the opportunity for the local community to understand the policy and for stakeholders and the community to participate in a scientific study, which is an excellent example of community-based participatory research, CBPR [25].
- HIAs can be conducted in a prospective, concurrent, or retrospective manner. This study was conducted with the recommended prospective method of assessment. Concurrent or retrospective HIAs provide opportunities for identifying previously unconsidered health impacts, whereas a prospective HIA allows for prediction of positive and negative impacts and makes it possible to modify the plans prior to actual implementation of the policy [10,26]. HIAs in Korea have mostly dealt with occurrences of environmental disease in a retrospective manner [27-30]. This study, however, is different, in that it evaluated the impacts on health prior to implementation and suggested the directions the policy should take.
- Another advantage of an HIA is that it provides an opportunity for intersectoral collaboration [12,31]. This study also entailed collaboration of public and private health institutions, experts and citizens, local and central government agencies, and with other local governments. It also required an interdisciplinary approach of collaboration of experts of health and GIS. Although this study focuses on a directly health-related issue, immunization, there are many more policies and projects of local governments in non-health sectors that are related to health, and an HIA can be an effective tool to consider the comprehensive health determinant factors in collaboration with relevant sectors [10,15,32]. However, it is not an easy task to explain the impact of health to non-experts, such as officials and citizens, in conducting an HIA. Assurance that the HIA is not a restrictive policy but a useful means of improving the quality of life of citizens by showing success stories and continuous understanding of the social determinants of health is essential.
- The underlying values of HIA are democracy, equity, sustainable development, and ethical use of evidence [7], of which equity is the most important. This implies that when an HIA identifies the distribution of the impacts of a policy on community health, the impacts on the vulnerable population must be prioritized. To consider the impact on the vulnerable population, this study included childcare facilities in the steering committee and the opinions of the staff were taken into account during the survey. The negative impacts and recommendations were considered from these comments.
- The limitations of this study include the small number of respondents from the surveys, a lack of comments from stakeholders and public hearings, and the absence of evaluation of the HIA, that is, change in policies, the results of the project, etc. However, the HIA that reviewed the Jinju Free Childhood Immunization Program from various perspectives is valuable in that it was the first HIA conducted by a local community on a health care issue, immunization, in Korea.
- HIA is one of the tools or procedures for developing healthy public policies [33,34]. This study systematically collected opinions on a policy implementation, the Jinju Free Childhood Immunization Program, according to the methods and procedures of an HIA and proposed recommendations. The results from this study can be used as evidence for future policies in Jinju. HIA is an approach that directly influences the decision-making process of public policy at the national or local government scale [10]. The Korea Institute for Health and Social Affairs translated methods and procedures developed in other countries and proposed a guideline for a simplified HIA for Korea [14]. However, more HIA cases need to be accumulated and produced to modify and fine-tune the Korean guidelines.
DISCUSSION
ACKNOWLEDGEMENTS
- 1. World Bank. World development report 1993: investing in health. 1993. Oxford: Oxford University Press; p. 8
- 2. Brownson RC, Baker EA, Leet TL, Gillespie KN. Evidence-based public health. 2003. Oxford: Oxford University Press; p. 146-147
- 3. Hinman AR, Orenstein WA, Schuchat A. Centers for Disease Control and Prevention (CDC). Vaccine-preventable diseases, immunizations, and MMWR: 1961-2011. MMWR Surveill Summ 2011;60(Suppl 4):49-57. 21976166
- 4. Kim YT. Demonstration project for expansion of NIP (National Immunization Program) coverage. J Korean Med Assoc 2005;48(6):579-586. (Korean)Article
- 5. Go UY. Expansion project for National Immunization Program coverage. J Korean Med Assoc 2007;50(8):660-661. (Korean)Article
- 6. Korea Center for Disease Control and Prevention. 2009 National financial assistance program for NIP. Public Health Wkly Rep 2010;3(48):1-4. (Korean)
- 7. European Centre for Health Policy. Health impact assessment: main concepts and suggested approach. Gothenburg consensus paper. 1999. Brussels: World Health Organization; p. 4
- 8. World Health Organization. Health impact assessment (HIA): examples of HIAs. cited 2012 Jul 16. Available from: http://www.who.int/hia/examples/en
- 9. Kang EJ, Lim SE. Improvement of child welfare service using health impact assessment: a case of the Cheongju Dream Start Center. Korean J Health Educ Promot 2011;28(1):115-130. (Korean)
- 10. Yoo WS, Kim KY, Koh KW. Introduction of health impact assessment and healthy cities as a tool for tackling health inequality. J Prev Med Public Health 2007;40(6):439-446. (Korean). 18063898ArticlePubMedPDF
- 11. Kim IS, Kim CG, Kang SH, Han SW. Studies for international trends in health impact assessment and linking HIA and EIA. J Environ Impact Assess 2005;14(5):275-289. (Korean)
- 12. Kang E, Park HJ, Kim JE. Health impact assessment as a strategy for intersectoral collaboration. J Prev Med Public Health 2011;44(5):201-209. 22020185ArticlePubMedPMCPDF
- 13. Scott-Samuel A, Birley MH, Ardern K. University of Liverpool, Department of Public Health. Merseyside Health Impact Assessment Steering Group. The Merseyside guidelines for health impact assessment. 2001. 2nd ed. Liverpool: IMPACT; p. 5-15
- 14. Kang EJ, Kim DJ, Park HJ. 2009 Health impact assessment system building and its operation. 2009. Seoul: Korean Institute for Health and Social Affairs; p. 1-354 (Korean)
- 15. Kemm J, Perry J. In: Kemm J, Parry J, Palmer S, editors. What is HIA? Introduction and overview. Health impact assessment: concepts, theory, techniques, and applications. 2005. Oxford: Oxford University Press; p. 15-23Article
- 16. Mindell J, Ison E, Joffe M. A glossary for health impact assessment. J Epidemiol Community Health 2003;57(9):647-651. 12933764ArticlePubMedPMC
- 17. Harris P, Harris-Roxas BE, Kemp L. Health impact assessment: a practical guide. 2007. cited 2012 Jul 16. Available from: http://www.hiaconnect.edu.au/files/Health_Impact_Assessment_A_Practical_Guide.pdf
- 18. Lee SH, Kim KC, Kim KM. A study on the service area for determining the size of general hospitals. J Korea Ins Healthc Archit 1996;1(2):73-81. (Korean)
- 19. Lee SG, Jeon SY, Kim YT, Lee JH, Kim YG, Lim MR. Experience on demonstration project for expansion of national immunization program coverage in Gunpho City, Korea. J Korean Soc Matern Child Health 2008;12(2):166-180. (Korean)Article
- 20. Lee JJ, Yang JH, Hwang IS, Chun BY, Kam S, Hwang TY, et al. The BCG, DTaP and IPV vaccination rate and the proportion of vaccination in the public health centers: demonstration project for expansion of national immunization program coverage in Daegu Metropolitan City. J Korean Soc Matern Child Health 2007;11(1):33-43. (Korean)
- 21. Lee SG, Jeon SY, Lee KS, Lee MS, Kim CB, Kim KY, et al. Evaluation of national burden project for essential national vaccination cost. 2010. Seoul: Korea Center for Disease Control and Prevention; p. 231-232 (Korean)
- 22. Pai MS. A study on the factors which influenced vaccination rate of infants in a city. Korean J Prev Med 1983;16(1):89-97. (Korean)
- 23. Jin SM, Lee SG. Vaccination status in school entry aged-children and associated factors on timeliness of vaccinations. J Korean Soc Matern Child Health 2007;11(1):44-53. (Korean)Article
- 24. Choi YK, Kim KY, Lee MS, Na BJ, Kim EY, Shim YB, et al. Timeliness of infant immunization rate at public health centers. J Korean Soc Matern Child Health 2008;12(2):181-198. (Korean)Article
- 25. Yoo SH. Using community-based participatory research (CBPR) for health promotion. J Korean Soc Health Educ Promot 2009;26(1):141-158. (Korean)
- 26. Taylor L, Blair-Stevens C. NHS Health Development Agency. Introducing health impact assessment (HIA): informing the decision-making process. 2002. London: Health Development Agency; p. 2-6
- 27. Lee KJ, Kim JJ, Choi HR, Yang GS, Kim H, Yim SH, et al. Health evaluation of ex-workers occupationally exposed to carbon disulfide: subjective symptoms and related factors according to compensation for CS2 poisoning. Korean J Occup Environ Med 2003;15(2):150-161. (Korean)ArticlePDF
- 28. Yun SH, Kim CY, Hwang TY, Won KC, Do JY, Lee SJ, et al. The concentration of cadmium in urine, and its role in health-risk assessment of residents in the vicinity of abandoned mines in Gyeongsangbuk-do, Korea. Korean J Occup Environ Med 2010;22(3):251-261. (Korean)ArticlePDF
- 29. Lee CH, Park KH, Lee MJ, Choi WH, Kim H, Park CH, et al. Health effect assessment on volunteers involved in the cleanup operation following the hebei spirit oil spill along the Taean coast, Korea. Korean J Occup Environ Med 2010;22(1):11-19. (Korean)ArticlePDF
- 30. Cho SY, Jang YS, Choi EK, Kim JS, Yu JY, Woo KH, et al. A case of peripheral polyneuropathy induced by occupational 2,5-hexanedione exposure. Korean J Occup Environ Med 2007;19(1):73-80. (Korean)ArticlePDF
- 31. Stead D. Institutional aspects of integrating transport, environment and health policies. Transp Policy 2008;15(3):139-148Article
- 32. Lock K. Health impact assessment. BMJ 2000;320(7246):1395-1398. 10818037ArticlePubMedPMC
- 33. Kemm J. Health impact assessment: an aid to political decision-making. Scand J Public Health 2008;36(8):785-788. 19004896ArticlePubMed
- 34. Mittelmark MB. Promoting social responsibility for health: health impact assessment and healthy public policy at the community level. Health Promot Int 2001;16(3):269-274. 11509463ArticlePubMed
REFERENCES
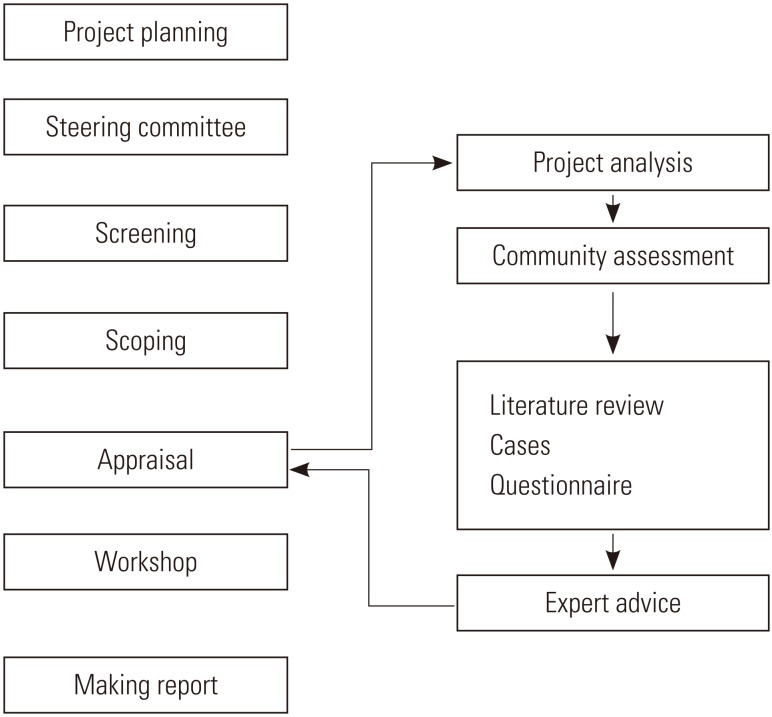
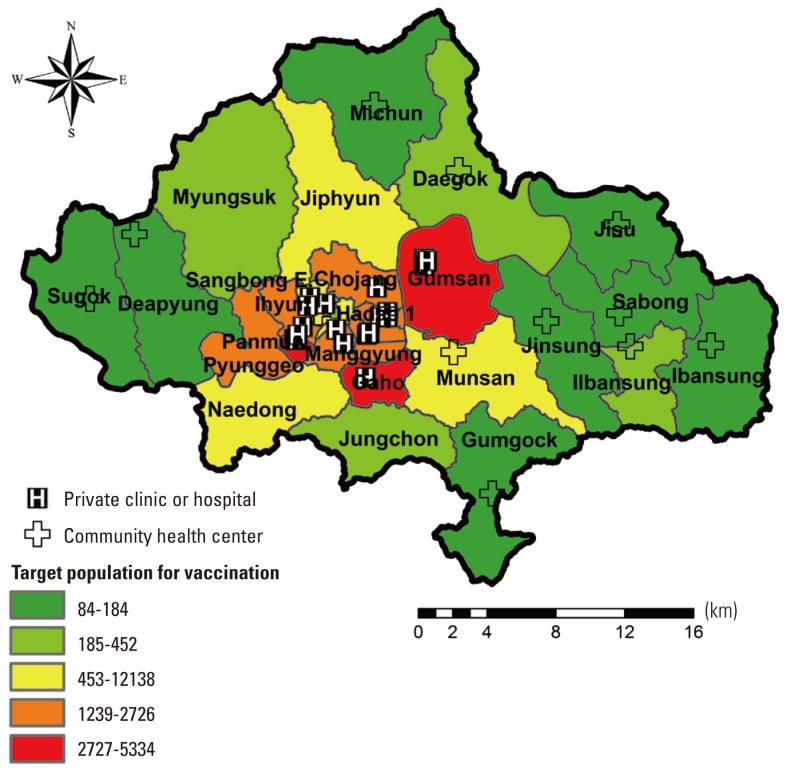
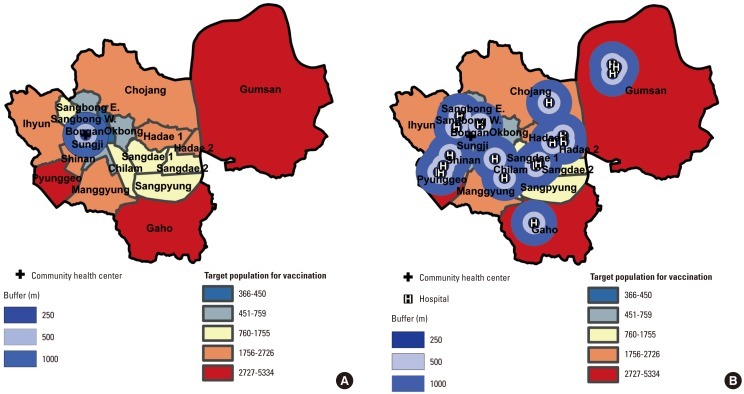
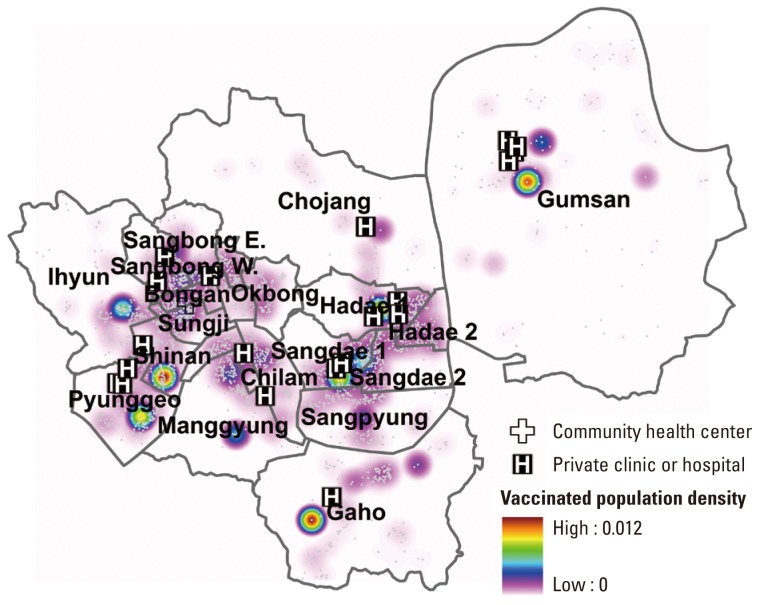
Figure & Data
References
Citations
- Cross-Sectional Study of Varicella Zoster Virus Immunity in Healthy Korean Children Assessed by Glycoprotein Enzyme-Linked Immunosorbent Assay and Fluorescent Antibody to Membrane Antigen Test
Yunhwa Kim, Ji-Young Hwang, Kyung-Min Lee, Eunsil Lee, Hosun Park
Vaccines.2021; 9(5): 492. CrossRef - Health Impact Assessments of Health Sector Proposals: An Audit and Narrative Synthesis
Nelius Wanjiku Wanjohi, Reema Harrison, Ben Harris-Roxas
International Journal of Environmental Research and Public Health.2021; 18(21): 11466. CrossRef - Epidemiological Impact of the Korean National Immunization Program on Varicella Incidence
Jaehun Jung, Young-Jin Ko, Young-Eun Kim, Kyungmin Huh, Byung-Joo Park, Seok-Jun Yoon
Journal of Korean Medical Science.2019;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite




