Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 52(3); 2019 > Article
-
Original Article
Non-linear Relationship Between Body Mass Index and Lower Urinary Tract Symptoms in Korean Males -
Chang Kyun Choi
 , Sun A Kim, Ji-An Jeong, Sun-Seog Kweon, Min-Ho Shin
, Sun A Kim, Ji-An Jeong, Sun-Seog Kweon, Min-Ho Shin -
Journal of Preventive Medicine and Public Health 2019;52(3):147-153.
DOI: https://doi.org/10.3961/jpmph.18.259
Published online: March 29, 2019
Department of Preventive Medicine, Chonnam National University Medical School, Hwasun, Korea
- Corresponding author: Min-Ho Shin, MD, PhD Department of Preventive Medicine, Chonnam National University Medical School, 264 Seoyang-ro, Hwasun 58128, Korea E-mail: mhshinx@paran.com
Copyright © 2019 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives:
- The purpose of this study was to evaluate the association between body mass index (BMI) and severe lower urinary tract symptoms (LUTS) in Korean males.
-
Methods:
- This study was conducted on males aged ≥50 years who participated in the 2011 Korean Community Health Survey. LUTS severity was assessed using the Korean version of the International Prostate Symptom Score (IPSS) questionnaire, and was dichotomized as severe (IPSS >19) and non-severe (IPSS ≤19). BMI was divided into 6 categories: <18.5, 18.5-22.9, 23.0-24.9, 25.0-27.4, 27.5-29.9, and ≥30.0 kg/m2. To evaluate the relationship between BMI and LUTS, a survey-weighted multivariate Poisson regression analysis was performed to estimate prevalence rate ratios (PRRs). Age, smoking status, alcohol intake, physical activity, educational level, household income, and comorbidities were adjusted for in the multivariate model.
-
Results:
- A U-shaped relationship was detected between BMI and severe LUTS. Compared with a BMI of 23.0-24.9 kg/m2, the PRR for a BMI <18.5 kg/m2 was 1.65 (95% confidence interval [CI], 1.35 to 2.02), that for a BMI of 18.5-22.9 kg/m2 was 1.25 (95% CI, 1.09 to 1.44), that for a BMI of 25.0-27.4 kg/m2 was 1.20 (95% CI, 1.00 to 1.45), that for a BMI of 27.5-29.9 kg/m2 was 1.11 (95% CI, 0.83 to 1.47), and that for a BMI ≥30.0 kg/m2 was 1.85 (95% CI, 1.18 to 2.88).
-
Conclusions:
- This study showed that both high and low BMI were associated with severe LUTS.
- Lower urinary tract symptoms (LUTS) refer to a combination of urinary symptoms associated with storage and/or voiding disturbance. Diseases such as spinal cord injury, prostate enlargement, and prostate cancer cause LUTS, and LUTS are also associated with cardiovascular risk factors, such as hypertension, dyslipidemia, and diabetes [1-3]. The prevalence of LUTS in Asian populations aged >60 years is >60% [4], and the incidence of prostate diseases, which are the main cause of LUTS in Korea, is increasing [5]. LUTS increase the public health burden by reducing quality of life (QoL) [6,7] and increasing the risk of falls and fracture [8,9].
- Many studies have investigated associations between obesity and LUTS, but the results have been inconsistent. In addition, the relevance of LUTS in underweight subjects has not been fully evaluated. Some previous studies have reported an association between obesity and LUTS [10-12], while others did not [13,14]. Additionally, most studies did not evaluate the relationship between underweight and LUTS. As LUTS and obesity are both strongly affected by lifestyle factors, such as diet, physical activity (PA), alcohol consumption, and smoking [10,12,15], a study with sufficient consideration of potential confounders is needed. The aim of this study was to evaluate the relationship between body mass index (BMI) and LUTS in Korean males aged 50 years or over. Specifically, we aimed to evaluate whether the relationship between BMI and LUTS was linear or non-linear, and to investigate the relationships of BMI categories based on World Health Organization cut-off points with LUTS.
INTRODUCTION
- Survey Design
- This study was conducted on males aged ≥50 years who participated in the 2011 Korean Community Health Survey (KCHS). The KCHS is a nationwide, cross-sectional survey carried out by the Korean Centers of Disease Control and Prevention [16]. The target population for the KCHS is adults aged ≥19 years who live within the jurisdiction of a community health center. The stratum was divided into 2 stages according to administrative units (dong, eup, and myeon) and housing units (apartments and houses), and the smallest administrative district units (tong, ban, and ri) were selected as the primary sampling unit of the stratum through probability proportionate sampling. Sample households were extracted through systemic sampling of the primary sampling units. Information was gathered through face-to-face interviews conducted by a trained interviewer. A total of 229 226 participants were enrolled in the 2011 KCHS, of whom 52 018 were males ≥50 years of age. BMI was missing for 1888 participants (3.6%), the International Prostate Symptom Score (IPSS) questionnaire was missing for 736 participants (1.4%), smoking status was missing for 8 participants (<0.1%), alcohol consumption was missing for 38 participants (0.1%), PA was missing for 183 participants (0.4%), marital status was missing for 37 participants (0.1%), household income was missing for 4049 participants (7.8%), education level was missing for 139 participants (0.3%), hypertension medication was missing for 23 participants (<0.1%), diabetes medication was missing for 35 participants (0.1%), and dyslipidemia medication was missing for 192 participants (0.4%). In the final analysis, 45 476 participants (87.4%) without missing values were included.
- Lower Urinary Tract Symptoms and Body Mass Index
- LUTS severity was assessed using the Korean version of the IPSS questionnaire [17], and dichotomized as severe (IPSS >19) and non-severe (IPSS ≤19) [18]. The IPSS questionnaire consists of 7 questions, on the following topics: frequency, urgency, nocturia, incomplete emptying, intermittency, weak stream, and straining to void. The scale of all items ranges from 0 to 5, and the higher the score, the more frequent the symptom. The IPSS storage subscore is the sum of the scores for the questions on frequency, urgency, and nocturia. The IPSS voiding subscore is the sum of the scores for the questions on incomplete emptying, intermittency, weak stream, and straining to void. BMI was calculated from self-reported body weight and height. BMI was divided into 6 categories: BMI<18.5, 18.5≤BMI<23.0, 23.0≤BMI< 25.0, 25.0≤BMI< 27.5, 27.5≤BMI<30.0, and BMI≥30.0 kg/m2 [19].
- Covariates
- Information on lifestyle factors, socioeconomic status, and comorbidities were collected through interviews. Alcohol consumption was coded as none, at least 1 standard drink per week, and less than 1 standard drink per week. Participants were classified by smoking status as current smokers, ex-smokers, and non-smokers. PA was dichotomized based on whether participants engaged in moderate or vigorous PA. Moderate PA was defined as moderate-intensity PA (e.g., swimming at a slow pace, table tennis, badminton, tennis doubles) for more than 5 days per week for 30 minutes or more. Vigorous PA was defined as vigorous-intensity PA (e.g., swimming at a fast pace, climbing, cycling, squash, tennis singles) for more than 3 days per week for 20 minutes or more. Marital status was coded as living with a partner or not. Household income was measured as self-reported monthly household income or annual household income and was divided into quartiles. Education level was categorized into primary school or no education and secondary or higher education. The presence of comorbidities, including hypertension, diabetes, dyslipidemia, and prostate enlargement, was determined by whether participants took medication for the disorder.
- Statistical Analysis
- The weighted baseline characteristics of the study population are expressed as mean±standard deviation or proportion (%). Linear regression analyses were performed to examine trends in the covariates across the BMI categories.
- Prevalence rate ratios (PRRs) according to BMI categories were estimated by multivariate Poisson regression, using svyglm from the survey package in R to account for the stratified multistage sampling design of the KCHS [20]. Four models were fit. Model 1 was crude, model 2 was adjusted for age, model 3 was additionally adjusted for socioeconomic status and lifestyle, and model 4 was additionally adjusted for comorbidities. The age-adjusted B-spline Poisson regression model was fitted using knots at the 5th, 50th, and 95th percentiles of BMI. Non-linearity was evaluated by comparing the goodness of fit of the B-spline regression model with the linear regression model.
- All results were weighted according to the sampling weights provided by the 2011 KCHS. Significance was set at a p-value <0.05. All analyses were performed using R version 3.5.1 (https://cran.r-project.org/bin/windows/base/old/3.5.1/).
METHODS
- The weighted baseline characteristics of the study population according to BMI category are presented in Table 1. Participants with higher BMIs were younger, had lower total IPSS and IPSS subscores, had a higher household income, more frequently resided with a partner, had more education, were less likely to be smokers, were more likely to be drinkers, engaged in more PA, and had higher prevalence rates of hypertension, diabetes, and dyslipidemia.
- Table 2 presents PRRs for severe LUTS according to BMI categories. A U-shaped relationship was detected between BMI and severe LUTS. The BMI category of 23.0-24.9 kg/m2 was used as the reference. In model 4, the PRR for a BMI <18.5 kg/m2 was 1.65 (95% confidence interval [CI], 1.35 to 2.02), that for a BMI of 18.5-22.9 kg/m2 was 1.25 (95% CI, 1.09 to 1.44), that for a BMI of 25.0-27.4 kg/m2 was 1.20 (95% CI, 1.00 to 1.45), that for a BMI of 27.5-29.9 kg/m2 was 1.11 (95% CI, 0.83 to 1.47), and that for a BMI ≥ 30.0 kg/m2 was 1.85 (95% CI, 1.18 to 2.88).
- Table 3 presents the results of a sensitivity analysis excluding subjects with prostate enlargement. The U-shaped relationship between BMI and severe LUTS was more prominent. In model 4, the PRR for a BMI <18.5 kg/m2 was 2.06 (95% CI, 1.57 to 2.70), that for a BMI of 18.5-22.9 kg/m2 was 1.42 (95% CI, 1.17 to 1.73), that for a BMI of 25.0-27.4 kg/m2 was 1.32 (95% CI, 1.02 to 1.71), that for a BMI of 27.5-29.9 kg/m2 was 1.26 (95% CI, 0.85 to 1.88), and that for a BMI ≥30.0 kg/m2 was 2.07 (95% CI, 1.14 to 3.73).
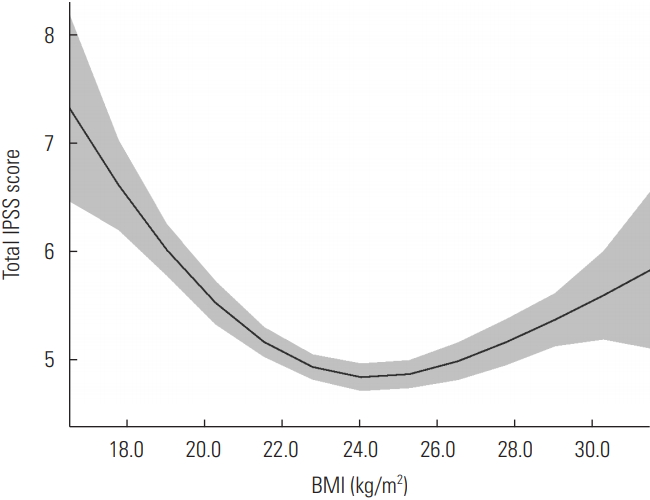
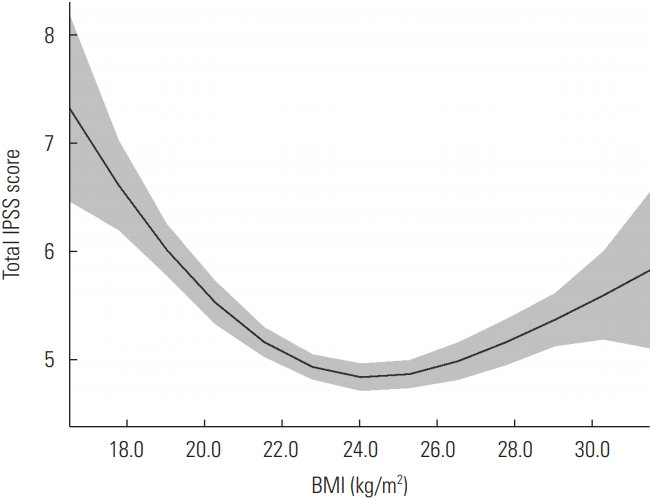
- Figure 1 shows the age-adjusted relationship between BMI and total IPSS. Data points below the 0.5th percentile and above the 99.5th percentile were removed as outliers. A U-shaped relationship was observed between BMI and IPSS (p for non-linearity <0.001). When the BMI was 24.0 kg/m2, the mean total IPSS was the lowest, at 4.85. The relationship between BMI and the IPSS subscores was also U-shaped (data not shown).
RESULTS
- In this large-scale cross-sectional study using a nationally representative sample of Korean adults, a U-shaped relationship was detected between BMI and LUTS, and the prevalence was lowest at a BMI of 23.0-24.9 kg/m2. The sensitivity analysis revealed that this relationship was more prominent in subjects without prostate enlargement. These results were independent of age, lifestyle, and comorbidities. This is the first study to show a non-linear relationship between BMI and LUTS.
- In previous studies on the associations between BMI and LUTS, a U-shaped association was not fully evaluated and the association was inconsistent. Most previous studies evaluated linear associations between BMI and LUTS [10,11,13] or did not evaluate the association between underweight and LUTS [12,14]. Chen et al. [10] reported that a high BMI was associated with a large prostate volume and a high IPSS in the Chinese population. Bhindi et al. [13] reported that BMI was not related to the IPSS, but was related to prostate volume. In the Third National Health and Nutrition Examination Survey, Rohrmann et al. [14] determined that current BMI was not associated with LUTS, but subjects who were obese and overweight at the age of 25 years had a low prevalence of LUTS. Associations between high BMI and LUTS have been reported in prospective studies. In the Boston Area Community Health Survey, Maserejian et al. [11] reported that a high BMI was associated with symptom progression. In the Osteoporotic Fractures in Men Study, Parsons et al. [12] reported a higher incidence of LUTS in subjects with overweight and obesity. In our study, a significant U-shaped relationship was observed between BMI and LUTS. Similar to our results, Smith et al. [21] reported a U-shaped relationship, with a high prevalence of severe LUTS found in individuals with obesity and underweight. However, no statistically significant differences were observed in the prevalence of LUTS between underweight and normal-weight participants because there were few underweight participants. In a study based on the 2012 KCHS, the relationship between BMI and overactive bladder was also U-shaped [22].
- The association between obesity and LUTS can be explained by hormonal changes. First, obesity induces insulin resistance, and the increased serum insulin elevates sympathetic nerve tone, leading to overactive bladder and prostate enlargement [23]. In addition, the androgen receptor located in the prostate smooth muscle binds insulin-like growth factor, so insulin can induce smooth muscle contraction [24]. Second, changes in sex hormones can exacerbate LUTS. Increased adipose tissue in obese subjects increases serum estrogen levels [25]. Estrogen is involved in the pathogenesis of prostate cancer, one of the causes of LUTS. In animal studies, estrogen has been found to act on estrogen receptor alpha, leading to prostate cancer [26]. In addition, higher testosterone-to-estrogen enzyme conversion activity resulted in a higher incidence of prostate cancer in a genome-wide association study [27].
- The mechanism for the relationship between underweight and LUTS is unclear, but a possible explanation is as follows. First, BMI reflects not only adiposity, but also lean body mass, and underweight is associated with sarcopenia [28]. Degradation of bladder function by sarcopenia or decreased muscle strength may be associated with voiding symptoms. In addition, the percentage of body fat may be high even in a subject with a low BMI because the percentage of muscle decreases with age [29]. LUTS can be induced by increased adipose tissue in both underweight and obesity. Second, the relationship between underweight and LUTS may reflect reverse causation. Poor QoL leads to weight loss [30], and LUTS deteriorates several indicators of QoL, such as sleep quality, depression, mobility, and self-rated health [31].
- The limitations of this study are as follows. First, we only used BMI as an index of obesity, but the relationships of underweight and obesity with LUTS have also been explored through other anthropometric methods, such as fat distribution, waist circumference, and the waist-hip ratio index. Second, BMI was calculated from self-reported body weight and height. In a study based on the 2016 KCHS, the correlation between measured BMI and BMI calculated by self-reported body weight and height was 0.86 at ages ≥60 years, which was lower than at other ages [32]. Therefore, further studies using accurately measured data are needed.
- In conclusion, a U-shaped relationship was detected between BMI and LUTS in Korean males, and this relationship was significant even after adjusting for lifestyle, socioeconomic status, and comorbidities. These results suggest that both underweight and obesity can contribute to LUTS. It also suggests that healthcare providers caring for LUTS patients need to pay attention to the issues of underweight and obesity. However, the role of underweight is unclear in the etiology of LUTS development. Further studies are needed on the mechanisms underlying this relationship.
DISCUSSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
Notes
| Characteristics |
BMI (kg/m2) |
p for trend | |||||
|---|---|---|---|---|---|---|---|
| <18.5 | 18.5-22.9 | 23.0-24.9 | 25.0-27.4 | 27.5-29.9 | ≥30.0 | ||
| Unweighted sample size (n) | 1830 | 18 989 | 13 352 | 8356 | 2379 | 570 | |
| Percentage of total sample | 2.9 | 40.1 | 30.6 | 19.7 | 5.5 | 1.3 | |
| Severe LUTS | 13.9 | 5.4 | 3.4 | 3.8 | 3.3 | 6.0 | <0.001 |
| Age | 69.4±0.4 | 62.1±0.1 | 60.5±0.1 | 59.6±0.1 | 58.9±0.2 | 58.6±0.5 | <0.001 |
| IPSS | |||||||
| Total | 8.84±0.30 | 4.88±0.07 | 4.03±0.07 | 3.96±0.09 | 3.89±0.15 | 4.33±0.38 | <0.001 |
| Voiding | 4.83±0.19 | 2.65±0.04 | 2.16±0.04 | 2.11±0.06 | 2.01±0.10 | 2.24±0.25 | <0.001 |
| Storage | 4.01±0.13 | 2.23±0.03 | 1.87±0.03 | 1.85±0.04 | 1.88±0.07 | 2.08±0.16 | <0.001 |
| Smoking history | <0.001 | ||||||
| Never | 15.0 | 19.2 | 21.2 | 20.0 | 20.6 | 18.6 | |
| Ex-smoker | 41.7 | 41.5 | 46.5 | 49.2 | 49.3 | 51.2 | |
| Current smoker | 43.4 | 39.3 | 32.3 | 30.8 | 30.1 | 30.2 | |
| Physical activity2 | 16.2 | 24.1 | 27.6 | 26.6 | 25.5 | 22.7 | <0.001 |
| Alcohol consumption (standard drink/d) | <0.001 | ||||||
| Non-drinker | 52.7 | 35.6 | 31.2 | 29.3 | 30.7 | 33.9 | |
| <1 | 18.9 | 28.8 | 30.2 | 29.4 | 26.4 | 21.7 | |
| ≥1 | 28.4 | 35.6 | 38.5 | 41.3 | 42.9 | 44.4 | |
| Living with partner | 82.6 | 86.6 | 89.8 | 89.9 | 89.9 | 90.3 | <0.001 |
| Household income | <0.001 | ||||||
| Q1 | 52.3 | 28.9 | 23.0 | 20.6 | 22.2 | 19.6 | |
| Q2 | 19.7 | 25.0 | 25.1 | 24.6 | 22.1 | 24.1 | |
| Q3 | 16.1 | 27.1 | 28.4 | 29.5 | 32.5 | 33.5 | |
| Q4 | 11.9 | 19.1 | 23.6 | 25.3 | 23.2 | 22.8 | |
| Higher than primary education | 56.6 | 76.3 | 82.1 | 83.3 | 82.6 | 80.3 | <0.001 |
| Hypertension | 19.8 | 24.6 | 31.8 | 39.9 | 46.6 | 60.0 | <0.001 |
| Diabetes | 8.4 | 11.2 | 13.1 | 15.3 | 17.3 | 23.8 | <0.001 |
| Dyslipidemia | 1.8 | 5.1 | 7.7 | 10.2 | 11.6 | 14.7 | <0.001 |
| Prostate enlargement | 12.0 | 7.7 | 7.5 | 7.4 | 7.3 | 8.7 | 0.076 |
Values are presented as % or mean±standard deviation.
BMI, body mass index; LUTS, lower urinary tract symptoms; IPSS, International Prostate Symptom Score.
1 All means, standard deviations, and percentages were calculated by using sampling weights.
2 Thirty minutes of moderate physical activity on 5 days or more per week.
|
BMI (kg/m2) |
||||||
|---|---|---|---|---|---|---|
| <18.5 | 18.5-22.9 | 23.0-24.9 | 25.0-27.4 | 27.5-29.9 | ≥30.0 | |
| Model 11 | 4.03 (3.31, 4.91) | 1.57 (1.36, 1.80) | 1.00 (reference) | 1.09 (0.90, 1.33) | 0.96 (0.72, 1.29) | 1.76 (1.14, 2.72) |
| Model 22 | 1.69 (1.38, 2.06) | 1.26 (1.10, 1.45) | 1.00 (reference) | 1.24 (1.02, 1.49) | 1.17 (0.88, 1.56) | 2.06 (1.30, 3.26) |
| Model 33 | 1.51 (1.23, 1.84) | 1.20 (1.05, 1.38) | 1.00 (reference) | 1.25 (1.03, 1.50) | 1.17 (0.88, 1.55) | 2.04 (1.31, 3.18) |
| Model 44 | 1.65 (1.35, 2.02) | 1.25 (1.09, 1.44) | 1.00 (reference) | 1.20 (1.00, 1.45) | 1.11 (0.83, 1.47) | 1.85 (1.18, 2.88) |
Values are presented as PRR (95% confidence interval).
PRR, prevalence rate ratio; LUTS, lower urinary tract symptoms; BMI, body mass index.
1 The crude model.
2 Adjusted for age.
3 Additionally adjusted for lifestyle factors (physical activity, alcohol consumption, and smoking status) and variables reflecting socioeconomic status (marital status, household income, and education level).
4 Additionally adjusted for comorbidities (hypertension, diabetes, and dyslipidemia).
|
BMI (kg/m2) |
||||||
|---|---|---|---|---|---|---|
| <18.5 | 18.5-22.9 | 23.0-24.9 | 25.0-27.4 | 27.5-29.9 | ≥30.0 | |
| Model 11 | 5.29 (4.07, 6.87) | 1.80 (1.48, 2.19) | 1.00 (reference) | 1.21 (0.93, 1.57) | 1.09 (0.73, 1.63) | 2.01 (1.12, 3.60) |
| Model 22 | 2.18 (1.67, 2.84) | 1.47 (1.20, 1.79) | 1.00 (reference) | 1.36 (1.05, 1.77) | 1.32 (0.89, 1.97) | 2.24 (1.22, 4.11) |
| Model 33 | 1.91 (1.46, 2.49) | 1.37 (1.13, 1.67) | 1.00 (reference) | 1.37 (1.05, 1.77) | 1.32 (0.89, 1.95) | 2.25 (1.25, 4.06) |
| Model 44 | 2.06 (1.57, 2.70) | 1.42 (1.17, 1.73) | 1.00 (reference) | 1.32 (1.02, 1.71) | 1.26 (0.85, 1.88) | 2.07 (1.14, 3.73) |
Values are presented as PRR (95% confidence interval).
PRR, prevalence rate ratio; LUTS, lower urinary tract symptoms; BMI, body mass index.
1 The crude model.
2 Adjusted for age.
3 Additionally adjusted for lifestyle factors (physical activity, alcohol consumption, and smoking status) and variables reflecting socioeconomic status (marital status, household income, and education level).
4 Additionally adjusted for comorbidities (hypertension, diabetes, and dyslipidemia).
- 1. Sarma AV, Parsons JK, McVary K, Wei JT. Diabetes and benign prostatic hyperplasia/lower urinary tract symptoms--what do we know? J Urol 2009;182(6 Suppl):S32-S37ArticlePubMed
- 2. Gibbons EP, Colen J, Nelson JB, Benoit RM. Correlation between risk factors for vascular disease and the American Urological Association Symptom Score. BJU Int 2007;99(1):97-100ArticlePubMed
- 3. Park JH, Cho IC, Kim YS, Kim SK, Min SK, Kye SS. Body mass index, waist-to-hip ratio, and metabolic syndrome as predictors of middle-aged men’s health. Korean J Urol 2015;56(5):386-392ArticlePubMedPMC
- 4. Chapple C, Castro-Diaz D, Chuang YC, Lee KS, Liao L, Liu SP, et al. Prevalence of lower urinary tract symptoms in China, Taiwan, and South Korea: results from a cross-sectional, population-based study. Adv Ther 2017;34(8):1953-1965ArticlePubMedPMCPDF
- 5. Han HH, Park JW, Na JC, Chung BH, Kim CS, Ko WJ. Epidemiology of prostate cancer in South Korea. Prostate Int 2015;3(3):99-102ArticlePubMedPMC
- 6. Robertson C, Link CL, Onel E, Mazzetta C, Keech M, Hobbs R, et al. The impact of lower urinary tract symptoms and comorbidities on quality of life: the BACH and UREPIK studies. BJU Int 2007;99(2):347-354ArticlePubMed
- 7. Coyne KS, Sexton CC, Irwin DE, Kopp ZS, Kelleher CJ, Milsom I. The impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int 2008;101(11):1388-1395ArticlePubMed
- 8. Gibson W, Hunter KF, Camicioli R, Booth J, Skelton DA, Dumoulin C, et al. The association between lower urinary tract symptoms and falls: forming a theoretical model for a research agenda. Neurourol Urodyn 2018;37(1):501-509ArticlePubMed
- 9. Noguchi N, Chan L, Cumming RG, Blyth FM, Naganathan V. A systematic review of the association between lower urinary tract symptoms and falls, injuries, and fractures in community-dwelling older men. Aging Male 2016;19(3):168-174ArticlePubMed
- 10. Chen Y, Yu W, Zhou L, Wu S, Yang Y, Wang J, et al. Relationship among diet habit and lower urinary tract symptoms and sexual function in outpatient-based males with LUTS/BPH: a multiregional and cross-sectional study in China. BMJ Open 2016;6(8):e010863ArticlePubMedPMC
- 11. Maserejian NN, Chen S, Chiu GR, Araujo AB, Kupelian V, Hall SA, et al. Treatment status and progression or regression of lower urinary tract symptoms in a general adult population sample. J Urol 2014;191(1):107-113ArticlePubMed
- 12. Parsons JK, Messer K, White M, Barrett-Connor E, Bauer DC, Marshall LM, et al. Obesity increases and physical activity decreases lower urinary tract symptom risk in older men: the Osteoporotic Fractures in Men Study. Eur Urol 2011;60(6):1173-1180ArticlePubMedPMC
- 13. Bhindi B, Margel D, Trottier G, Hamilton RJ, Kulkarni GS, Hersey KM, et al. Obesity is associated with larger prostate volume but not with worse urinary symptoms: analysis of a large multiethnic cohort. Urology 2014;83(1):81-87ArticlePubMed
- 14. Rohrmann S, Smit E, Giovannucci E, Platz EA. Associations of obesity with lower urinary tract symptoms and noncancer prostate surgery in the Third National Health and Nutrition Examination Survey. Am J Epidemiol 2004;159(4):390-397ArticlePubMedPDF
- 15. Kristal AR, Arnold KB, Schenk JM, Neuhouser ML, Weiss N, Goodman P, et al. Race/ethnicity, obesity, health related behaviors and the risk of symptomatic benign prostatic hyperplasia: results from the prostate cancer prevention trial. J Urol 2007;177(4):1395-1400ArticlePubMed
- 16. Kang YW, Ko YS, Kim YJ, Sung KM, Kim HJ, Choi HY, et al. Korea Community Health Survey data profiles. Osong Public Health Res Perspect 2015;6(3):211-217ArticlePubMedPMC
- 17. Choi HR, Chung WS, Shim BS, Kwon SW, Hong SJ, Chung BH, et al. Translation validity and reliability of I-PSS Korean version. Korean J Urol 1996;37(6):659-665. (Korean)
- 18. D’Silva KA, Dahm P, Wong CL. Does this man with lower urinary tract symptoms have bladder outlet obstruction? The rational clinical examination: a systematic review. JAMA 2014;312(5):535-542ArticlePubMed
- 19. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004;363(9403):157-163ArticlePubMed
- 20. Lumley T. Analysis of complex survey samples. J Stat Softw 2014;9(1):1-19Article
- 21. Smith DP, Weber MF, Soga K, Korda RJ, Tikellis G, Patel MI, et al. Relationship between lifestyle and health factors and severe lower urinary tract symptoms (LUTS) in 106,435 middle-aged and older Australian men: population-based study. PLoS One 2014;9(10):e109278ArticlePubMedPMC
- 22. Kim SY, Bang W, Choi HG. Analysis of the prevalence and associated factors of overactive bladder in adult Korean men. PLoS One 2017;12(4):e0175641ArticlePubMedPMC
- 23. Rohrmann S, Platz EA, Giovannucci E. Lifestyle and benign prostatic hyperplasia in older men: what do we know? J Mens Health Gend 2005;2(2):230-235Article
- 24. Sayeed A, Alam N, Trerotola M, Languino LR. Insulin-like growth factor 1 stimulation of androgen receptor activity requires β(1A) integrins. J Cell Physiol 2012;227(2):751-758ArticlePubMedPMC
- 25. Vermeulen A, Kaufman JM, Giagulli VA. Influence of some biological indexes on sex hormone-binding globulin and androgen levels in aging or obese males. J Clin Endocrinol Metab 1996;81(5):1821-1826ArticlePubMed
- 26. Ricke WA, McPherson SJ, Bianco JJ, Cunha GR, Wang Y, Risbridger GP. Prostatic hormonal carcinogenesis is mediated by in situ estrogen production and estrogen receptor alpha signaling. FASEB J 2008;22(5):1512-1520ArticlePubMed
- 27. Cussenot O, Azzouzi AR, Nicolaiew N, Fromont G, Mangin P, Cormier L, et al. Combination of polymorphisms from genes related to estrogen metabolism and risk of prostate cancers: the hidden face of estrogens. J Clin Oncol 2007;25(24):3596-3602ArticlePubMed
- 28. Lauretani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, Di Iorio A, et al. Age-associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol (1985) 2003;95(5):1851-1860ArticlePubMed
- 29. Roubenoff R. Sarcopenia and its implications for the elderly. Eur J Clin Nutr 2000;54 Suppl 3: S40-S47ArticlePubMedPDF
- 30. Hulman A, Ibsen DB, Laursen AS, Dahm CC. Body mass index trajectories preceding first report of poor self-rated health: a longitudinal case-control analysis of the English Longitudinal Study of Ageing. PLoS One 2019;14(2):e0212862ArticlePubMedPMC
- 31. Nuotio M, Tammela TL, Luukkaala T, Jylhä M. Association of urgency symptoms with self-rated health, mood and functioning in an older population. Aging Clin Exp Res 2007;19(6):465-471ArticlePubMedPDF
- 32. Jeong JY, Kim DH, Kim KY, Ryu SY, Lee SY, Park YS. Accuracy of self-reported height, weight and body mass index in Community Health Survey in South Korea. J Health Info Stat 2017;42(3):241-249. (Korean)ArticlePDF
REFERENCES
Figure & Data
References
Citations
- Metabolic syndrome and male lower urinary tract symptoms
Gallus B. INEICHEN, Fiona C. BURKHARD
Panminerva Medica.2022;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite