
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 54(2); 2021 > Article
-
Original Article
The Burden of Stroke in Kurdistan Province, Iran From 2011 to 2017 -
Shahram Moradi
 , Ghobad Moradi, Bakhtiar Piroozi
, Ghobad Moradi, Bakhtiar Piroozi -
Journal of Preventive Medicine and Public Health 2021;54(2):103-109.
DOI: https://doi.org/10.3961/jpmph.20.335
Published online: February 1, 2021
Social Determinants of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj, Iran
- Corresponding author: Ghobad Moradi Social Determinants of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, P.O.Box 66177-13446, Sanandaj, Iran E-mail: moradi_gh@yahoo.com
Copyright © 2021 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- The aim of this study was to calculate the burden of stroke in Kurdistan Province, Iran between 2011 and 2017.
-
Methods
- Incidence data extracted from the hospital information system of Kurdistan Province and death data extracted from the system of registration and classification of causes of death were used in a cross-sectional study. The World Health Organization method was used to calculate disability-adjusted life years (DALYs).
-
Results
- The burden of stroke increased from 2453.44 DALYs in 2011 to 5269.68 in 2017, the years of life lost increased from 2381.57 in 2011 to 5109.68 in 2017, and the years of healthy life lost due to disability increased from 71.87 in 2011 to 159.99 in 2017. The DALYs of ischaemic stroke exceeded those of haemorrhagic stroke. The burden of disease, new cases, and deaths doubled during the study period. The age-standardised incidence rate of ischaemic stroke and haemorrhagic stroke in 2017 was 21.72 and 20.72 per 100 000 population, respectively.
-
Conclusions
- The burden of stroke is increasing in Kurdistan Province. Since health services in Iran are based on treatment, steps are needed to revise the current treatment services for stroke and to improve the quality of services. Policy-makers and managers of the health system need to plan to reduce the known risk factors for stroke in the community. In addition to preventive interventions, efficient and up-to-date interventions are recommended for the rapid diagnosis and treatment of stroke patients in hospitals. Along with therapeutic interventions, preventive interventions can help reduce the stroke burden.
- Stroke is a major public health problem that represents a significant proportion of the global burden of disease [1]. More than 13.7 million new cases of stroke were estimated worldwide in 2016 [2]. Stroke was also the second leading global cause of death in the same year, after ischaemic heart disease [3]. More than 80% of stroke-induced deaths occur in developing countries [4]. Although preventive strategies have reduced the burden of stroke [5], the December 2017 report of the United Nations General Assembly argued that the decline in the burden of non-communicable diseases, including neurological disorders, has not been enough to achieve the Sustainable Development Goals by 2030. Based on age-standardised disability-adjusted life years (DALYs), stroke burden decreased from 1990 to 2016; however, the absolute number of strokes increased in the same period. This increase is mostly due to the aging and growing population [3]. Stroke in Iran creates a heavy burden of disease. In 2016, there were an estimated 82 516 new cases of stroke and 28 786 stroke-induced deaths in Iran [3]. Some studies in provinces of Iran have shown burden of disease for stroke. Ghandehari et al. [6] estimated the incidence of stroke in Khorasan Province between 2001 and 2005 to be 43.12 per 100 000 people annually. Ahangar et al. [7] found that the incidence of stroke in Babol between 2001 and 2003 was 50 per 100 000. The ultimate goal of estimating the burden of diseases is to provide highly objective evidence required for policy-making [8]. There have not been many studies aiming to calculate the burden of stroke in Iran in recent years. However, one study used modelling to estimate the nation-wide burden of stroke in 2003 in Iran [9]. Many studies conducted throughout the world have used modelling to estimate the burden of stroke, although this method has limitations [10,11]. The distinctive feature of this study is that it used data from stroke and death registration systems, unlike many modelling-based studies of disease-specific DALYs for which researchers did not have access to data from disease and mortality registration systems. Model-based estimates are not as accurate as estimates made using registration systems. In addition, in this study, DALYs were calculated separately for ischaemic and haemorrhagic stroke. The stroke registration system in Iran was launched after 2011 in hospitals. Everyone who experiences a stroke usually goes to the hospital, so the system records almost all stroke cases. Since the data of the registration systems were available from 2011 onward and no study in Kurdistan Province—and even Iran more broadly—has calculated the burden of this disease in recent years separately for haemorrhagic and ischaemic stroke using data from stroke and death registration systems, the present study was conducted to calculate the burden of stroke in Kurdistan Province. The findings can provide accurate knowledge about the burden of this disease in a sample of the Iranian population.
INTRODUCTION
- This cross-sectional study was conducted in 2019 in all age groups in Kurdistan Province based on the population data of the province between 2011 and 2017. Kurdistan Province is a mountainous provinces in the west of Iran at the Iran-Iraq border. The population of the province was 1 600 000 in 2016, including 149 000 older adults. This number is rising. Most of the residents of the province are of Kurdish ethnicity with unique culture and customs. The disease burden was calculated using the global disease burden calculation method and DALYs, which are calculated using the sum of the years of life lost due to premature mortality (YLL) and the years of healthy life lost due to disability (YLD). One DALY is the equivalent of 1 year of life that should be spent in health, but is lost either due to premature death or disability due to illness or injury. The higher the figure, the worse the disease is or the less likely that it is controlled by the health system [12]. Few studies have calculated DALYs separately for haemorrhagic and ischaemic stroke. In addition, to the best of our knowledge, this study is the first study to calculate the burden of stroke over a period of 7 years in Iran using the stroke and death registration systems. YLD was calculated as the product of stroke incidence and disability weight considering the course of the disease. To calculate YLL due to premature mortality, the number of people who died due to stroke was multiplied by the life expectancy of the age group. In this study, DALYs were calculated according to sex, 8 age groups (0-4, 5-14, 15-29, 30-44, 45-59, 60-69, 70-79, and ≥80 years), and the year of stroke incidence. The incidence of stroke and death was calculated separately for ischaemic and haemorrhagic strokes according to International Statistical Classification of Diseases and Related Health Problems-10th revision (ICD-10) codes, as follows: ischaemic stroke: G45-G46.8, I63-I63.9, I65-I66.9, I67.2-I67.3, I67.5-I67.6, I69.3. and haemorrhagic stroke: I60-I62.9, I67.0-I67.1, I68.1-I68.2, I69.0-I69.2.
- The annual crude incidence of ischaemic stroke was calculated as follows: A/B×100 000=16.57, where A is the number of new cases of ischaemic stroke per year (1856/7=265.14) and B is the population of Kurdistan (1 600 000). To calculate the crude incidence of stroke, the number of strokes was divided by the total population in the province in that year and reported per 100 000 individuals. To calculate the crude death rate, the total number of deaths was divided by the total population of the province in that year. The age-standardised incidence rate (ASIR) was also calculated based on the standard population. Specific disability weights for age groups were used in this study, as 0.258 for the 60+ age group and 0.224 for all other age groups [13]. Data on the incidence of stroke were obtained from hospitals, where stroke patients need specialised care due to the severity of the condition. As a result, the stroke registration system is hospital-based in most countries A hospital-based stroke registration system has been implemented in Iran, including Kurdistan Province, since 2011. In the Iranian health system, patients who present to the hospital with suspected symptoms of stroke are examined by a general practitioner or emergency physician and then referred to a neurologist. After confirmation by a neurologist, the type of disorder is classified in terms of ICD-10 codes and registered in the stroke registration system. The population of Kurdistan Province in each year was extracted separately from the website of the Statistics Centre of Iran, and the data covered all the inhabitants of the province. The mortality data were extracted from the Registration and Classification System of the Causes of Death. Iran has a death registration system to record deaths and causes of death. Therefore, the stroke and death registration systems of Kurdistan Province were the most important data sources for this study. However, in the final data, duplicates were removed based on ICD-10 codes and year of admission. The 2 components of the DALY index were calculated based on the following formula:
- DALY=YLL+YLD
- YLL=N×L
- YLD=I×DW×D
- Where N is the number of deaths, L is life expectancy, I is incidence, D is disease period, and DW is the disability weight.
- Ethics Statement
- The Ethics Committee of Kurdistan University of Medical Sciences (IR.MUK.REC.1397/203) approved this study.
METHODS
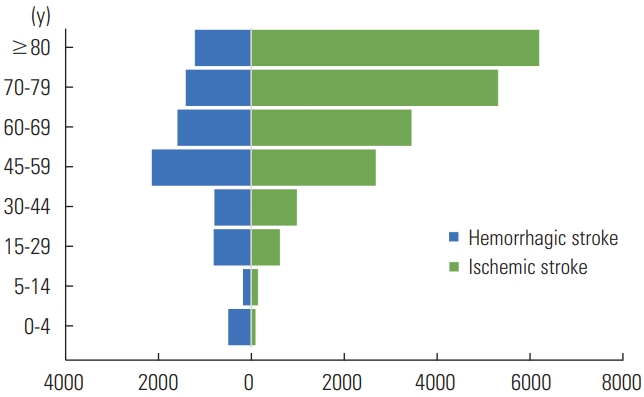
- The incidence of new cases and deaths in both men and women doubled by 2017 compared to 2011 (Table 1). The burden of stroke increased from 2453.44 DALYs in 2011 to 5269.68 DALYs in 2017. The YLL and YLD for ischaemic stroke were 18 867.62 and 460.13, respectively, while those figures for haemorrhagic stroke were 7918.60 and 615.40, respectively. The DALYs of ischaemic stroke exceeded those of haemorrhagic stroke. The DALYs of stroke were higher in men than in women. In both types of stroke, YLL surpassed YLD (Figure 1). The ASIR of ischaemic stroke in men and women was 22.81 and 20.63 per 100 000 population, respectively. The ASIR of haemorrhagic stroke in men and women was 24.20 and 17.46 per 100 000 population, respectively (Table 2). The burden of disease for ischaemic stroke increased with age, with the highest burden observed in the age group over 80 years. For haemorrhagic stroke, the highest burden was seen in the age group of 45-59 years; in the age groups above this category, the burden decreased, most likely due to the high mortality rate of this condition (Figure 2).
RESULTS
- To the best of our knowledge, this is the first study to calculate the burden of diseases in Iran over a 7-year period using data from the stroke and death registration systems. The numbers of YLLs and YLDs over this period were 26 786.22 (96.0%) and 1075.53 (4.0%), respectively; indicating a very high mortality rate for stroke. The total DALYs for ischaemic and haemorrhagic stroke were 19 327.75 and 8534.00, respectively. Moreover, the total DALYs of stroke in men and women were 16 145.63 and 11 716.13, respectively. Based on the results of the study, the burden of stroke has increased over time.
- The ASIR for ischaemic stroke was higher than that for haemorrhagic stroke, which is consistent with the results of various studies in recent years and is similar to the pattern observed in developed countries [14-17]. This is more evident compared to most African countries, where the ASIR for haemorrhagic stroke is higher than that for ischaemic stroke [18]. It seems that the increasing trend of stroke-induced DALYs in Kurdistan Province is due to the increase in life expectancy and population aging. Moreover, the burden of stroke was higher in men than in women, which is consistent with the results of various studies [2,18,19]. The number of YLLs was higher than that of YLDs, which is consistent with previously reported results [20,21]. This may be an indication of poor services in the emergency treatment and stroke care systems. Therefore, rapid identification of patients and immediate interventions can reduce the number of deaths. At the same time, policy-makers and managers of the health system should take the necessary measures to reduce the risk factors for stroke. Health systems in developed countries have created special wards in hospitals, called stroke units, for rapid treatment interventions for stroke that prevent dangerous complications. Moreover, the burden of stroke in the age groups under 40 years was low in Kurdistan Province and followed a pattern similar to that in other countries. As age increases, the mortality rate rises and consequently DALYs increase. This indicates that the age pattern of stroke in this study was similar to that of most countries of the world, with death from stroke before the age of 40 being rare. In our study, the annual crude incidence of ischaemic stroke was 16.57 per 100 000 people, which is inconsistent with the results of the study of Ghandehari et al. [6] in Khorasan Razavi Province (43.17 per 100 000 people). This inconsistency may be due to differences in the quality of the stroke registration system, differences in age pattern, or differences in risk factors for the disease. In our study, the DALYs of stroke in 2016 were 268 per 100 000 people, which is inconsistent with the national average in the same year (776 per 100 000). This may be due to differences in the prevalence of risk factors for stroke, differences in calculation methods, and differences in disease registration methods. The burden of stroke in Kurdistan Province in 2017 was 5269.68 DALYs. Compared to the results of a study by Johnston et al. [11] in the same year in 193 countries, the burden of stroke of Kurdistan Province was higher than that in 23 countries, including countries in Southeast Asia, Western Europe, the Caribbean, and Oceania [3]. One of the reasons for this is the population growth and aging in Kurdistan Province. The burden of ischaemic stroke in 2017 was 336 DALYs per 100 000 people, which based on the results of Krishnamurthi et al. [22], is consistent with that of Bahrain (301) and the United States (295) and inconsistent with that of Iraq (991), Jordan (881), Kazakhstan (1339), Kuwait (731), Lebanon (470), Pakistan (548), and Turkey (876). The reasons for this inconsistency can be attributed to an increase in life expectancy [13], an increasing trend in population aging [23], a decrease in the age of stroke [24], better pre-hospital and nursing services, and better post-stroke care, which have led to an increase in the number of YLDs and eventually DALYs. In more developed countries and cities, immediate deaths and complications are prevented by creating stroke units and performing immediate interventions. These interventions reduce immediate mortality.
- Given that the causes of stroke are hypertension and smoking [21,25-28] and considering that the prevalence of hypertension and smoking in Kurdistan Province is higher than the national average (the WHO STEPwise approach to surveillance [STEPS] 2016), the burden of stroke in Kurdistan Province seems underestimate. Population-based stroke registration programs can help making better estimates. Since stroke is the second leading cause of death worldwide, and the burden of stroke increased during the study period, policy-makers should consider the burden of stroke and steps should be taken to provide appropriate facilities for prevention, rapid treatment, and rehabilitation. The high prevalence of key risk factors for stroke such as smoking, hypertension, lack of proper physical activity, increased life expectancy, and population aging has contributed to the increased stroke burden in Kurdistan Province. Health policymakers and managers must plan to reduce these risk factors in the general population. In addition to preventive interventions, essential and up-to-date interventions are recommended for the rapid diagnosis and treatment of stroke in hospitals.
- The solution for reducing the death rate and severe disabilities caused by stroke is to increase access to fast and up-todate diagnostic and treatment services. In addition, proper rehabilitation of improved patients can help reduce DALYs by reducing the severity of complications. One of the limitations of this study is the quality of stroke registration system data. As the data from the early years of the study period coincide with the beginning of the integration of this stroke registration system, the data may have been affected by underestimation bias, especially in the early years.
- In conclusion, the burden of stroke is increasing in Kurdistan Province. Given that health services in Iran are based on treatment, steps must be taken to revise the current treatment services for stroke and to improve the quality of services. Policymakers and managers of the health system must introduce plans to reduce the known risk factors of this disease in the community. In addition to preventive interventions, essential and up-to-date interventions are recommended for the rapid diagnosis and treatment of stroke in hospitals. Along with therapeutic interventions, stroke prevention interventions can help reduce the DALYs lost due to stroke.
DISCUSSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
Kurdistan University of Medical Sciences funded this study.
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Conceptualization: SM, GM. Data curation: SM. Formal analysis: SM. Funding acquisition: GM. Methodology: SM, GM, BP. Project administration: SM, GM, BP. Visualization: SM. Writing – original draft: SM. Writing – review & editing: SM, GM, BP.
Notes

- 1. O’Donnell M, Xavier D, Diener C, Sacco R, Lisheng L, Zhang H, et al. Rationale and design of INTERSTROKE: a global casecontrol study of risk factors for stroke. Neuroepidemiology 2010;35(1):36-44ArticlePubMed
- 2. GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019;18(5):459-480PubMedPMC
- 3. GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019;18(5):439-458PubMedPMC
- 4. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet 2006;367(9524):1747-1757ArticlePubMed
- 5. Langhorne P, O’Donnell MJ, Chin SL, Zhang H, Xavier D, Avezum A, et al. Practice patterns and outcomes after stroke across countries at different economic levels (INTERSTROKE): an international observational study. Lancet 2018;391(10134):2019-2027PubMed
- 6. Ghandehari K, Izadi Z; Khorasan Stroke Registry. The Khorasan Stroke Registry: results of a five-year hospital-based study. Cerebrovasc Dis 2007;23(2-3):132-139ArticlePubMed
- 7. Ahangar AA, Vaghefi SB, Ramaezani M. Epidemiological evaluation of stroke in Babol, northern Iran (2001-2003). Eur Neurol 2005;54(2):93-97ArticlePubMed
- 8. Karikari TK, Charway-Felli A, Höglund K, Blennow K, Zetterberg H. Commentary: global, regional, and national burden of neurological disorders during 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Front Neurol 2018;9: 201ArticlePubMedPMC
- 9. Naghavi MO, Abolhassani F, Pourmalek FA, Jafari NA, Moradi Lakeh M, Eshrati B, et al. The burden of disease and injury in Iran in the year 2003. Iran J Epidemiol 2008;4(1):1-19. (Persian)
- 10. Roth GA, Johnson CO, Nguyen G, Naghavi M, Feigin VL, Murray CJ, et al. Methods for estimating the global burden of cerebrovascular diseases. Neuroepidemiology 2015;45(3):146-151ArticlePubMed
- 11. Johnston SC, Mendis S, Mathers CD. Global variation in stroke burden and mortality: estimates from monitoring, surveillance, and modelling. Lancet Neurol 2009;8(4):345-354ArticlePubMed
- 12. Zaletel-Kragelj L, Boz̆ ikov J; Forum for Public Health in South Eastern Europe. Methods and tools in public health: a handbook for teachers, researchers, and health professionals. Lage: Hans Jacobs; 2010. p. 715-748
- 13. World Health Organization. The global burden of disease: 2004 update. [cited 2020 Jul 1]. Available from: https://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/
- 14. Bahonar A, Khosravi A, Khorvash F, Maracy M, Oveisgharan S, Mohammadifard N, et al. Ten-year trend in stroke incidence and its subtypes in Isfahan, Iran during 2003-2013. Iran J Neurol 2017;16(4):201-209PubMedPMC
- 15. Wang YL, Wu D, Liao X, Zhang W, Zhao X, Wang YJ. Burden of stroke in China. Int J Stroke 2007;2(3):211-213ArticlePubMed
- 16. Feigin VL, Mensah GA, Norrving B, Murray CJ, Roth GA; GBD 2013 Stroke Panel Experts Group. Atlas of the global burden of stroke (1990-2013): the GBD 2013 study. Neuroepidemiology 2015;45(3):230-236ArticlePubMedPMC
- 17. Feigin VL, Krishnamurthi RV, Parmar P, Norrving B, Mensah GA, Bennett DA, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: the GBD 2013 study. Neuroepidemiology 2015;45(3):161-176ArticlePubMedPMC
- 18. Owolabi MO, Akarolo-Anthony S, Akinyemi R, Arnett D, Gebregziabher M, Jenkins C, et al. The burden of stroke in Africa: a glance at the present and a glimpse into the future. Cardiovasc J Afr 2015;26(2 Suppl 1):S27-S38ArticlePubMedPMC
- 19. Kusuma Y, Venketasubramanian N, Kiemas LS, Misbach J. Burden of stroke in Indonesia. Int J Stroke 2009;4(5):379-380ArticlePubMed
- 20. Gao Y, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. The burden of stroke in China: results from a nationwide population-based epidemiological survey. PLoS One 2018;13(12):e0208398ArticlePubMedPMC
- 21. Lee H, Yoon SJ, Ahn HS, Moon OR. Estimation of potential health gains from reducing multiple risk factors of stroke in Korea. Public Health 2007;121(10):774-780ArticlePubMed
- 22. Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of firstever ischaemic and haemorrhagic stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet Glob Health 2013;1(5):e259-e281ArticlePubMedPMC
- 23. Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ; Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet 2002;360(9343):1347-1360ArticlePubMed
- 24. Katan M, Luft A. Global burden of stroke. Semin Neurol 2018;38(2):208-211ArticlePubMed
- 25. Dean N, Shuaib A. Hypertension: the most important preventable risk factor for cerebrovascular disease. Lancet Neurol 2011;10(7):606-607Article
- 26. Romero JR, Wolf PA. Epidemiology of stroke: legacy of the Framingham Heart Study. Glob Heart 2013;8(1):67-75ArticlePubMedPMC
- 27. Gorelick PB. The global burden of stroke: persistent and disabling. Lancet Neurol 2019;18(5):417-418ArticlePubMed
- 28. Wajngarten M, Silva GS. Hypertension and stroke: update on treatment. Eur Cardiol 2019;14(2):111-115ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


