
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 55(4); 2022 > Article
-
Original Article
Inequality in Private Health Care Expenditures: A 36-Year Trend Study of Iranian Households -
Ehsan Aghapour1
 , Mehdi Basakha1,2, Seyed Hossein Mohaqeqi Kamal1,3, Abolghasem Pourreza4
, Mehdi Basakha1,2, Seyed Hossein Mohaqeqi Kamal1,3, Abolghasem Pourreza4 -
Journal of Preventive Medicine and Public Health 2022;55(4):379-388.
DOI: https://doi.org/10.3961/jpmph.22.123
Published online: June 27, 2022
1Department of Social Welfare Management, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
2Social Determinants of Health Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
3Social Welfare Management Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran
4Department of Health Management and Economics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
- Corresponding author: Mehdi Basakha, Department of Social Welfare Management, University of Social Welfare and Rehabilitation Sciences, Kodakyar Avenue, Tehran 1985713871, Iran, E-mail: Me.basakha@uswr.ac.ir
Copyright © 2022 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- Throughout history, societies have been impacted by inequality. Many studies have been conducted on the topic more broadly, but only a few have investigated inequalities in out-of-pocket health payments (OHP). This study measures OHP inequality trends among the Iranian households.
-
Methods
- This study used data from the Iranian Statistics Center on Iranian household income and expenditures. The analysis included a total of 995 300 households during the 36 years from 1984 to 2019. The Gini coefficient, Atkinson index, and Theil index were calculated for Iranian OHP.
-
Results
- Average Iranian household OHP increased from 33 US dollar (USD) in 1984 to 47 USD in 2019. During this 36-year span, the average±standard deviation Gini coefficient for OHP was 0.73±0.04, and the Atkinson and Theil indexes were 0.68±0.05 and 1.14±0.29, respectively. The Gini coefficients for the subcategories of OHP of outpatient diagnostic services, medical assistant accessories, hospital inpatient services, and addiction cessation were 0.70, 0.61, 0.84, and 0.64, respectively.
-
Conclusions
- In this study, we scrutinized trends of inequality in the OHP of Iranian households. Inequality in OHP decreased slightly over the past four decades. An analysis of trends among different subgroups revealed that affluent households, such as households with insurance coverage and households in higher income deciles, experienced higher inequality. Therefore, lower inequality in health care expenditures may be related to restricted access to health care services in Iran.
- A key concern for policymakers has been providing households with financial support for health care services [1,2]. To address this concern, systems involving out-of-pocket health payments (OHP) have been introduced, and their importance has steadily grown in many countries [1,3]. Health care services are commonly financed through a combination of taxation, social health insurance, private health insurance, community financing, and OHP [4,5].
- OHP may combat the phenomenon known as “moral hazard,” whereby households might use less necessary or unnecessary health services too frequently when they are free of charge, whereas household contributions could reduce this. OHP can also serve as a source of health care financing [1,6]. One way to measure fairness in health care financing is by analyzing OHP [7]. A high proportion of OHP can be considered a threat to a health care financing system, since relying on a high-risk source can limit the availability of health services for epidemics or life changes such as aging. While OHP overall is an issue that requires more attention, studying OHP inequality is the more critical aspect, because an unequal distribution of OHP can divert family income away from essential needs such as food, education, shelter, and utilities [8–10]. Numerous studies have calculated inequality in well-being indicators such as income, wealth and consumption, or various indicators of health, such as access to services [11]. In Iran, OHP is a major source of health care financing [5,12,13], and evidence shows that health care expenditures have been increasing over the decades [14–16].
- Inequality in OHP has become an increasing health policy challenge for many countries [17,18]. The health care system in Iran was formed from the principles of the Conference of Alma Ata, namely access to health services for all, a focus on primary care and prevention, attention to disadvantaged groups, and investments in public health workers. The system is a public/private partnership, with the public health sector funded by public expenditures, including direct government spending, and reimbursement from the Iranian Social Security Organization and Health Insurance Organization [19]. In 2018, health system funding in Iran consisted of government expenditures (about 24%), social health insurance (about 31%), direct OHP (about 35%), private health insurance (about 6%), and other sources (about 4%), with health care expenditures accounting for 8.4% of Iran’s gross domestic product [20].
- Indicators of inequality in health expenditures have been widely studied by Iranian researchers, but this study is the first to address the issue comprehensively over a 36-year timeframe [5,21]. Mehrolhassani et al. [22] reported that the distribution of health care expenditures was unequal, especially in OHP, with the highest rate ranging from 0.50 to 0.59 during the study timeframe and the disparity index for OHP fluctuating between 37.01% and 65.85%. Bock et al. [1] reported a mean OHP over three months of €119, with 34% for medical supplies, 22% for dental prostheses, 21% for pharmaceuticals, 17% for outpatient physician and non-physician services, 5% for inpatient care, and 1% for nursing care. In Iran, there is some limited evidence on inequality trends in health care expenditures, particularly Ghaedamini et al. [23] who studied inequality in Iranian household expenditures over a decade. The Gini coefficient (GC) in their study was unusually high for health care expenditures, averaging 0.78. The current study uses the GC as well but has also added two more refined indicators of inequality, the Theil and Atkinson indexes. These incorporate additional qualitative criteria such as inequality aversion and entropy when calculating inequality indexes [24]. This study also considered inequality in OHP among different socio-demographic subgroups. The findings, therefore, make a significant contribution to the understanding of health inequalities and provide valuable input for policymakers in Iran aiming to ensure more equity in health care. In summary, this study measured the trends in inequality indexes for Iranian household OHP over 36 years, and further analyzed this inequality based on household income ranges and insurance coverage status.
INTRODUCTION
- Data
- This study used data from the Household Income and Expenditure Survey gathered annually by the Statistical Center of Iran. The analysis included a total of 995 300 households over the 36 years from 1984 to 2019. Among Iranian households, OHP (also referred to as out-of-pocket expenditures or co-payments) are paid in 1 of 3 ways: deductibles, or amounts paid for covered health care expenditures before insurance starts paying, additional payments triggered when a stipulated insurance threshold is reached, and direct contributions to health care services, including for outpatient diagnostic services, equipment, supplies, medical assistant accessories, hospital inpatient service, and addiction cessation [25]. This study used Stata version 14.2 (StataCorp., College Station, TX, USA) to analyze the data, with the INEQDECO Stata module used to estimate the full range of inequality indexes [26].
- Measures
- Inequality in household expenditures was measured using 3 different indicators: the GC, the Theil index of inequality (with its sensitivity to disparities at the top and the bottom of the OHP distribution), and the Atkinson index of inequality (with 2 parameters for inequality aversion).
- The GC has many desirable characteristics as a measure of inequality, including mean and population size independence symmetry and Pigou-Dalton transfer sensitivity. The GC ranges from 0 to 1, where 0 indicates perfect equality (all individuals have the same resources) and 1 indicates perfect inequality (where one person has all the resources and the rest have none). The closer the GC is to 1, therefore, the more unequal the population and vice-versa. Focusing on the GC as a measure of inequality allows comparisons of inequalities in health care expenditures over time and space [27]. Its cumulative frequency curve compares the distribution of total health care expenditures yi with the cumulative percentage of population xi. The GC was calculated using the formula [27,28] of Haughton as shown in equation (1):
- where N is the total number of observations. If N is equal to the interval on the x-axis, the GC can be simplified to equation (2):
- The Atkinson index shows the percentage of total resources that a population would have to forego in order to have more equal shares of income between the individuals. Atkinson (1970) approached inequality from a normative perspective and proposed welfare-based inequality measures called Atkinson’s class measures A(ɛ). The parameter(ɛ) represents aversion to inequality and has values between zero and infinity. The larger the parameter(ɛ), the stronger the inequality aversion in a society. This means that the Atkinson index is more sensitive to the bottom of the income/expenditure distribution [29]. A greater aversion parameter(ɛ) indicates that social welfare is more sensitive to a shift in the income of a poorer individual than to the same shift for a richer individual [30].
- The Theil index was also calculated for OHP among Iranian households. The Theil index is a generalized entropy inequality measure, GE(ɲ). The parameter ɲ represents the weight given to distances between income/expenditure at different parts of the income/expenditure distribution. The parameter ɲ can take any real value, with commonly used values of 0, 1, and 2. When ɲ is equal to 0, the GE(0) index is called the Theil L index, when ɲ is equal to 1, the GE(1) index is called the Theil T index, and when ɲ is equal to 2, the GE(2) index is called the coefficient of variation [31]. With a large and positive ɲ, the GE index is more sensitive to changes at the upper tail of the income/expenditure distribution, while with ɲ values closer to zero, the GE index is more sensitive to changes at the bottom tail of the distribution.
- Ethics Statement
- This research was in accordance with the ethical standards of the Committee of Ethics in Research in the University of Social Welfare and Rehabilitation Sciences and approved by ethical code: IR. USWRREC.1398.201.
METHODS
- Profile of Iranian Households
- Historically, the heads of most Iranian households have been men (around 90%), while more recently there has been a slight increase in women-headed households (from 10.1% in 1984 to 14.3% in 2019). During this period, the rate of insurance coverage also increased rapidly from 26.6% in 1984 to 88.8% in 2019. The proportions of urban and rural households during this time were consistent, with only slight fluctuations. The literacy rate for heads of households increased considerably from 51.0% in 1984 to 75.5% in 2019. Household size has also dropped over the years, from an average of 5.1 persons per household in 1994 to 3.4 in 2019. Since 2011, health care expenditures have grown at least 12% year over year (Tables 1 and 2).
- Inequality in Out-of-pocket Health Payments
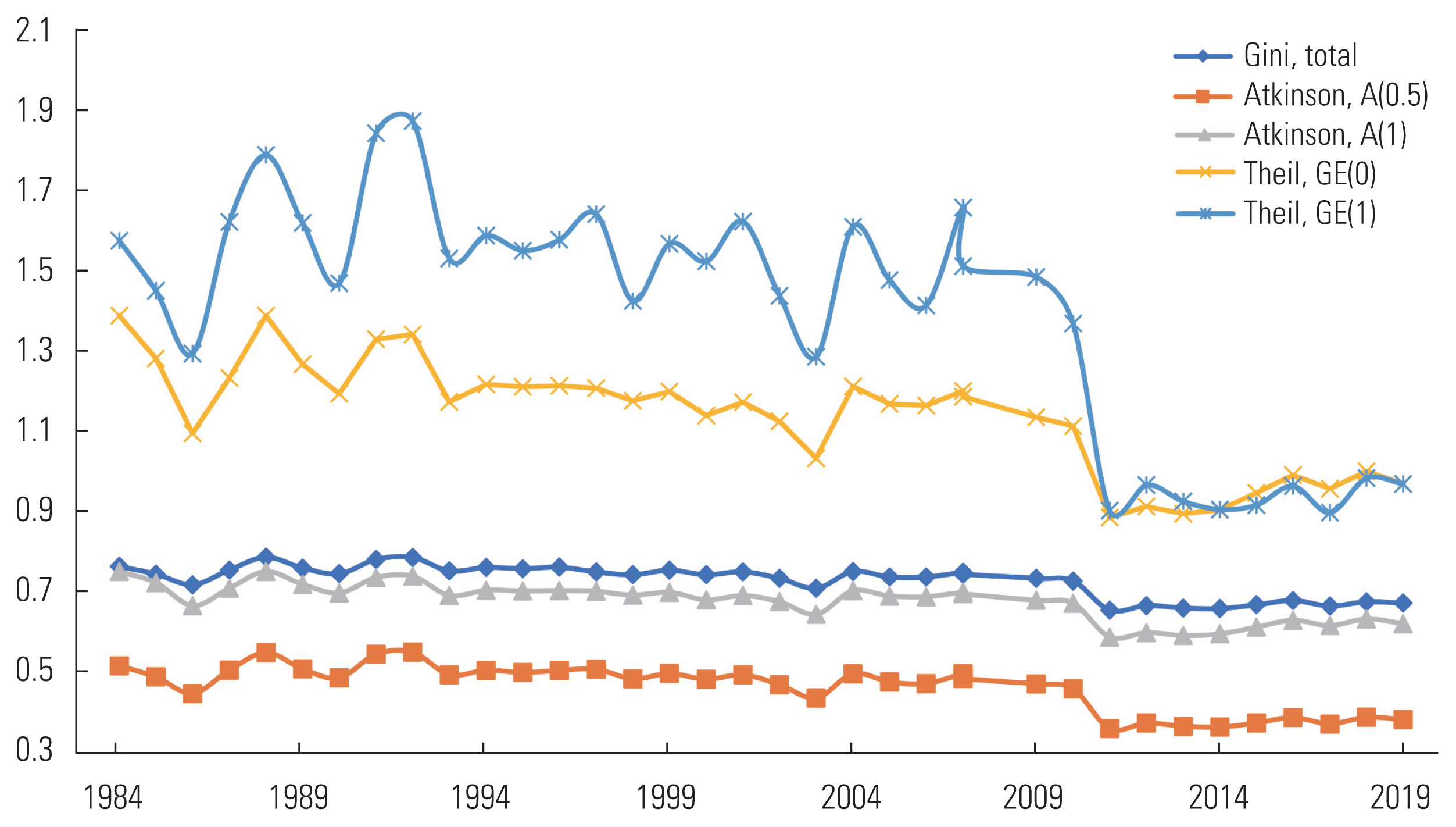
- Using the annual data on Iranian household health expenditures, inequality indexes were calculated over the 36 years. All inequality measures showed inequality slowly declining from 1984 to 2019. The one exception was 2010, when all the measures suddenly dropped. Inequality in OHP then remained mostly constant until 2019. During this period, the mean±standard deviation (SD) of the GC was 0.73±0.04, with a minimum and maximum of 0.65 and 0.78 in the years 2011 and 1988, respectively. The mean±SD of the Atkinson index for inequality among Iranian households was A(0.5)=0.46±0.06. Focusing on the OHP of the lowest income group, the Atkinson index is higher with the mean A(1)=0.68±0.05. Similarly, Figure 1 shows the trends for the Thiel index of inequality using the inequality aversion parameters 1 and 0. Over the 36-year period, the average for GE(1) and GE(0) was 1.39±0.29 and 1.14±0.14, respectively. It is clear that more sensitivity to inequalities at the top of the OHP distribution has led to higher levels of inequality. This is evidenced by the fact that inequality was much more pronounced among households with higher OHP. In 2010 the inequality converged for both inequality aversion parameters, most likely indicating that households with better economic conditions were less able to meet their health needs.
- Figure 2 shows the inequality trend in OHP among sample subgroups (note that data for expenditures on addiction cessation are only available for 2005 onward). The mean of the GCs for expenditures on equipment, supplies, and medical assistant accessories was 0.61±0.02, suggesting it was the least important factor measured here affecting inequality in health care expenditures. The mean of the GC for outpatient diagnostic services expenditures was 0.70±0.01, with the coefficient at its highest level in 1995 (0.74). Among all the components of OHP, hospital services expenditures had the highest level of inequality (0.84±0.08). Inequality in expenditures for addiction cessation, despite a few peturbations, was almost constant.
- The mean GCs were 0.74±0.05 for households covered by insurance and 0.71±0.04 for those without insurance coverage (Table 3). The trend of inequality had slight fluctuations before 2011, but in 2011 it dropped significantly, and inequality between the 2 groups of households has since converged. Table 3 also gives the GCs for different income deciles, to help understand differences in inequality between households with different income levels. The OHP was highly unequal in the topmost decile subgroup, with a mean GC for 1984 to 2019 of 0.75±0.05. All deciles showed decreased inequality in 2011, with the mean of GCs for the bottom decile (first) of 0.70±0.06.
RESULTS
- This study calculated inequality measures in OHP among Iranian households over 36 years and provided a breakdown of inequality trends. All inequality indicators showed slightly decreases in OHP inequality in line with previous studies [16,31]. A similar trend of declining inequality in health spending has been reported in some other countries. According to Çinaroğlu [32], GC results indicated decreasing inequality in OHP expenditures between 2003 (0.75), 2009 (0.71), and 2015 (0.69). The level of progressivity decreased from 2003 to 2015, with less progressivity in distribution of OHP expenditures [32].
- The highest inequality has been detected in hospital services expenditures (Figure 2), with outpatient diagnostic services and equipment and medical supplies showing a relatively smooth trend over the 36 years. Ghaedamini et al. [23] showed that Iranian households experienced severe inequality in health care expenditures. The present study found that the highest level of inequality was among households with insurance coverage as well as households in the tenth income decile. More access to health care services, often facilitated by insurance coverage and high income, appeared to be an important factor in this higher inequality in health care spending.
- To understand the overall status of inequality in health care expenditures, all the observed trends should be analyzed simultaneously. In 2011 there was a sudden and significant decline in all measures of inequality. The Theil index showed that an important part of this reduction in inequality was related to households with higher health expenditures. This analysis has also shown that inequality in hospital spending has decreased significantly. It appears that households with insurance coverage and higher incomes have become more similar in terms of inequality to households without insurance coverage and with lower incomes. Households that used to experience higher inequality in health care expenditures, namely high-income and insurance-covered households, are now experiencing declining inequality. Reduced household spending inequality should be distributed unequally because of unequal health needs. The observed reductions, however, may be a result of limited access to health care services, especially expensive hospital services. In 2011, the Iranian economy experienced a shock in foreign exchange rates that destroyed the purchasing power of Iranian households. This sharp decline in real incomes has made health care services more unaffordable for families [33] especially for those with extensive needs, such as people with disabilities and families with other specialized needs. According to Rezapour et al. [34], economic problems are making patients less likely to seek out medical services, with Kordbache and Ahmadi [35] showing that the exchange rate has significant and direct impacts on medical care prices both in the short and long term. They showed effects of exchange rate changes on medical care price indexes for consumers and producers of 0.23 and 0.14 in the short term and 0.327 and 0.256 in the long term, respectively. Atkinson index values show the proportion of total OHP which would be required to achieve an level of social welfare equal to the present state if expenditures were perfectly distributed. The mean Atkinson index values of A(0.5)= 0.46 and A(1)=0.68 suggest that Iran’s health system could achieve the same level of social welfare with only 1−0.46=0.54 and 1−0.68=0.32 the amount of current OHP. In the last decade, the “target subsidies plan” was implemented in Iran with the aim of reducing government subsidies in the economy. This plan started in 2010 and sought to expand government funding for social insurance and health care services, as well as affordable medical care for specific diseases. The high inflationary effects of this policy [36], however, worsened the inequality in health care financing and made access to health care services more limited than before. Reducing the inequality in household OHP was considered auspicious in previous study [37], but the current study showed that high inequality in health spending was related to affluent families (households with insurance coverage and high-income households) in society. As a result, inequality should be interpreted cautiously in counties with high OHP shares in health care expenditures.
- This study used a large raw data set from Iranian households to calculate inequality indexes. The measures of inequality included the GC and the Theil and Atkinson indexes. For the first time, a long-term trend of for inequality was established and analyzed based on households’ income decile and insurance coverage status. The data suggest that implementation of the “targeted subsidies plan” and the following exchange rate shock has reduced inequality in OHP since 2011. The higher inequality rates seen for households with higher socioeconomic status suggest that lowering inequality in Iran may have been due to limited access to health care services. The trend of inequality indexes as well as more detailed analysis of the 36 years of data reinforce this viewpoint. A significant reduction in the inequality of hospital services’ expenditures, for example, suggests that some households in need of expensive medical services may have been deprived of these services, possibly with devastating health consequences. This study provides a time series of data that can be used for further health inequality analysis.
DISCUSSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
None.
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Conceptualization: Aghapour E, Basakha M. Data curation: Aghapour E, Basakha M. Formal analysis: Aghapour E, Basakha M, Mohaqeqi Kamal SH. Funding acquisition: None. Methodology: Aghapour E, Basakha M, Pourreza A. Project administration: Basakha M. Writing – original draft: Aghapour E, Basakha M. Writing – review & editing: Aghapour E, Basakha M, Mohaqeqi Kamal SH, Pourreza A.
Notes

- 1. Bock JO, Matschinger H, Brenner H, Wild B, Haefeli WE, Quinzler R, et al. Inequalities in out-of-pocket payments for health care services among elderly Germans--results of a population-based cross-sectional study. Int J Equity Health 2014;13: 3ArticlePubMedPMC
- 2. Organization for Economic Cooperation and Development (OECD). Health data; 2022 [cited 2022 Mar 5]. Available from: http://www.oecd.org/health/healthdata
- 3. Tambor M, Pavlova M, Woch P, Groot W. Diversity and dynamics of patient cost-sharing for physicians’ and hospital services in the 27 European Union countries. Eur J Public Health 2011;21(5):585-590ArticlePubMed
- 4. Gottret P, Schieber G. Health financing revisited: a practitioner’s guide; 2006 [cited 2021 Oct 17]. Available from: https://openknowledge.worldbank.org/handle/10986/7094
- 5. Rezaei S, Woldemichael A, Ebrahimi M, Ahmadi S. Trend and status of out-of-pocket payments for healthcare in Iran: equity and catastrophic effect. J Egypt Public Health Assoc 2020;95(1):29ArticlePubMedPMCPDF
- 6. Corrieri S, Heider D, Matschinger H, Lehnert T, Raum E, König HH. Income-, education- and gender-related inequalities in out-of-pocket health-care payments for 65+ patients - a systematic review. Int J Equity Health 2010;9: 20ArticlePubMedPMC
- 7. Pourasghari H, Jafari M, Bakhtiari M, Keliddar I, Irani A, Afshari M. Analysis of equality in Iranian household healthcare payments during Iran’s fourth development program. Electron Physician 2016;8(7):2645-2649ArticlePubMedPMC
- 8. Ekholuenetale M, Barrow A. Inequalities in out-of-pocket health expenditure among women of reproductive age: after-effects of national health insurance scheme initiation in Ghana. J Egypt Public Health Assoc 2021;96(1):6ArticlePubMedPMCPDF
- 9. Akazili J, McIntyre D, Kanmiki EW, Gyapong J, Oduro A, Sankoh O, et al. Assessing the catastrophic effects of out-of-pocket healthcare payments prior to the uptake of a nationwide health insurance scheme in Ghana. Glob Health Action 2017;10(1):1289735ArticlePubMedPMCPDF
- 10. Kanmiki EW, Bawah AA, Phillips JF, Awoonor-Williams JK, Kachur SP, Asuming PO, et al. Out-of-pocket payment for primary healthcare in the era of national health insurance: evidence from northern Ghana. PLoS One 2019;14(8):e0221146ArticlePubMedPMC
- 11. O’Donnell O, van Doorslaer E, Wagstaff A, Lindelow M. Analyzing health equity using household survey data: a guide to techniques and their implementation; 2008 [cited 2021 Oct 17]. Available from: https://openknowledge.worldbank.org/handle/10986/6896
- 12. Chu A, Kwon S, Cowley P. Health financing reforms for moving towards universal health coverage in the Western Pacific Region. Health Syst Reform 2019;5(1):32-47ArticlePubMed
- 13. Fakhri MA, Juni MH, Rosliza AM. Assesing progressivity of out-of-pocket expenditures for health care: evidence from households in Malaysia. Int J Public Health Clin Sci 2019;6(3):187-202
- 14. Hajimahmoudi H, Zahedi F. Justice in the healthcare system: payment and reimbursement policies in Iran. Iran J Med Ethics Hist Med 2014;6(3):1-16. (Persian)
- 15. Abolhallaje M, Mousavi SM, Jafari M. Implementation of performance-based budgeting in the health system: luxury or necessity? Iran J Public Health 2014;43(11):1593-1594PubMedPMC
- 16. Hajimahmoudi H, Zahedi F. Justice in the healthcare system: payment and reimbursement policies in Iran. Iran J Med Ethics Hist Med 2013;6(3):1-16. (Persian)PubMed
- 17. Murray CJ, Knaul F, Musgrove P, Xu K, Kawabata K. Defining and measuring fairness in financial contribution to the health system; GPE Discussion Paper Series: No. 24. 2000 [cited 2021 Dec 12]. Available from: https://apps.who.int/iris/handle/10665/68706
- 18. Jafari M, Bastani P, Ibrahimipour H, Dehnavieh R. Attitude of health information system managers and officials of the hospitals regarding the role of information technology in reengineering the business procedures: a qualitative study. HealthMED 2012;6(1):208-215
- 19. Bazyar M, Rashidian A, Alipouri Sakha M, Vaez Mahdavi MR, Doshmangir L. Combining health insurance funds in a fragmented context: what kind of challenges should be considered? BMC Health Serv Res 2020;20(1):26ArticlePubMedPMCPDF
- 20. Doshmangir L, Rashidian A, Kouhi F, Gordeev VS. Setting health care services tariffs in Iran: half a century quest for a window of opportunity. Int J Equity Health 2020;19(1):112ArticlePubMedPMCPDF
- 21. Jalali FS, Jafari A, Bayati M, Bastani P, Ravangard R. Equity in healthcare financing: a case of Iran. Int J Equity Health 2019;18(1):92ArticlePubMedPMCPDF
- 22. Mehrolhassani MH, Yazdi-Feyzabadi V, Lashkari M. Measuring inequalities in the selected indicators of National Health Accounts from 2008 to 2016: evidence from Iran. Cost Eff Resour Alloc 2020;18: 37ArticlePubMedPMCPDF
- 23. Ghaedamini GH, Sharifian Sani M, Raghfar H, Salehi M. Inequality trend of selected items of consumption household basket in Tehran: 1989–2006. Soc Welf Q 2011;11(40):315-339. (Persian)
- 24. Kawachi I, Subramanian SV, Almeida-Filho N. A glossary for health inequalities. J Epidemiol Community Health 2002;56(9):647-652ArticlePubMedPMC
- 25. Statistical Center of Iran. Household, Expenditure and Income Survey; 2022 [cited 2021 Jun 6]. Available from: https://www.amar.org.ir/english/Statistics-by-Topic/Household-Expenditure-and-Income#2220530-releases
- 26. Jenkins SP. INEQDECO: Stata module to calculate inequality indices with decomposition by subgroup; 2001 [cited 2021 Feb 22]. Available from: https://ideas.repec.org/c/boc/bocode/s366007.html
- 27. Haughton J, Khandker SR. Handbook on poverty and inequality; 2009 [cited 2021 Oct 12]. Available from: https://openknowledge.worldbank.org/handle/10986/11985
- 28. Raghfar H, Zargari N, Sangari MK. Measuring inequality in households’ health care expenditures in Iran. Hakim Res J 2013;16(2):89-97. (Persian)
- 29. Statistics South Africa. Inequality trends in South Africa: a multidimensional diagnostic of inequality; 2019 [cited 2021 Oct 12]. Available from: http://www.statssa.gov.za/publications/Report-03-10-19/Report-03-10-192017.pdf
- 30. Tregenna F, Tsela M. Inequality in South Africa: the distribution of income, expenditure and earnings. Dev South Afr 2012;29(1):35-61Article
- 31. Ghiasvand H, Naghdi S, Abolhassani N, Shaarbafchizadeh N, Moghri J. Iranian households’ payments on food and health out-of-pocket expenditures: evidence of inequality. Iran J Public Health 2015;44(8):1103-1113PubMedPMC
- 32. Çinaroğlu S. Inequality and inequity in financing out-of-pocket health expenditures: an applied econometric approach. J Bus Res Turk 2018;10(1):876-897
- 33. Zandian H, Takian A, Rashidian A, Bayati M, Zahirian Moghadam T, Rezaei S, et al. Effects of Iranian economic reforms on equity in social and healthcare financing: a segmented regression analysis. J Prev Med Public Health 2018;51(2):83-91ArticlePubMedPMCPDF
- 34. Rezapour A, Mahmoudi M, Gorji HA, Faradonbeh SB, Asadi S, Zadeh NY, et al. A survey of Unmet health needs and the related barriers to access them. J Health Adm 2014;17(57):87-98. (Persian)
- 35. Kordbache H, Ahmadi Z. Evaluation the effect of exchange rate fluctuations on medical care price indexes in Iran. J Healthc Manag 2018;8(4):17-27. (Persian)
- 36. Noferesti M, Jalouli M. Analyzing the impact of the removal of basic commodity subsidies on the main macroeconomic variables within a structural macro econometric framework. J Econ Model 2010;1(1):81-105. (Persian)
- 37. Jalali FS, Jafari A, Bayati M, Bastani P, Ravangard R. Equity in healthcare financing: a case of Iran. Int J Equity Health 2019;18(1):92ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
- Decomposition of Healthcare Utilization Inequality in Iran: The Prominent Role of Health Literacy and Neighborhood Characteristics
Neda Soleimanvandiazar, Seyed Hossein Mohaqeqi Kamal, Mehdi Basakha, Salah Eddin Karimi, Sina Ahmadi, Gholamreza Ghaedamini Harouni, Homeira Sajjadi, Ameneh Setareh Forouzan
INQUIRY: The Journal of Health Care Organization, Provision, and Financing.2024;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


