Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 57(2); 2024 > Article
-
Original Article
Knowledge, Attitudes, and Practices Regarding Dengue Prevention Among Health Volunteers in an Urban Area – Malang, Indonesia -
Alidha Nur Rakhmani1
 , Lilik Zuhriyah2
, Lilik Zuhriyah2 -
Journal of Preventive Medicine and Public Health 2024;57(2):176-184.
DOI: https://doi.org/10.3961/jpmph.23.484
Published online: February 21, 2024
- 1,710 Views
- 139 Download
1Department Family Medicine, Faculty of Medicine, Universitas Brawijaya, Malang, Indonesia
2Department Public Health, Faculty of Medicine, Universitas Brawijaya, Malang, Indonesia
- Corresponding author: Alidha Nur Rakhmani, Department Family Medicine, Faculty of Medicine, Universitas Brawijaya, Jl. Veteran, Malang 65145, Indonesia E-mail: alidha@ub.ac.id
Copyright © 2024 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives:
- The dengue prevention program known as “One House One Mosquito Larva Inspector” involves health volunteers who play a crucial role in the surveillance of mosquito larvae and reporting their findings to local public health officials. This study aimed to identify factors related to the knowledge, attitudes, and practices (KAP) of dengue prevention behavior among these health volunteers.
-
Methods:
- A study was conducted in 5 sub-districts in Malang, an urban area in Indonesia. We employed a cross-sectional design and utilized a semi-structured questionnaire to assess the KAP of 400 health volunteers. Data were collected through face-to-face interviews.
-
Results:
- Multiple logistic regression analysis revealed that individuals with a more positive attitude (odds ratio [OR], 1.69; p<0.05) and those with family sizes greater than five persons (OR, 1.90; p<0.05) were more likely to engage in effective dengue prevention practices. Additionally, possesing good knowledge was significantly assocated with more positive attitude (OR, 2.24; p<0.001). Furthermore, 40% reduction in positive attitude was observed in those over 45 years (OR, 0.60; p<0.05). The best practices most frequently reported by the majority of respondents included always reporting their surveillance activities (75.8%) and cleaning the water container in the bathroom at least once a week (65.2%). However, only 52.2% of respondents regularly checked for mosquito larvae in their neighborhood.
-
Conclusions:
- Sustainable promotion and training for the “One House One Mosquito Larva Inspector” initiative are necessary, particularly among young health volunteers, to improve dengue prevention behaviors both within their own homes and in the surrounding environment.
- Dengue remains a health challenge in East Java, Indonesia, including in Malang. Given that Malang is an urban region, there is a higher chance of dengue cases there due to the increased risk of dengue transmission based on earlier research [1]. Malang, the second-largest city in East Java, has seen a consistent increase in dengue cases year over year. In 2015, there were 335 reported cases of dengue with 3 fatalities, and in 2016, the number of cases rose to 446, with 2 deaths reported [2,3].
- Dengue fever prevention programs in Indonesia include surveillance systems, case management, vector control, and initiatives to change people’s behavior. Vector control efforts are integrated with behavior change strategies through a surveillance system known as “3M Plus,” which encourages the community to periodically combat mosquito breeding sites. Despite these efforts, the incidence of dengue cases remains high [4-6]. In 2016, the Indonesian Ministry of Health launched the Healthy Indonesia Program, which aims to improve health services by adopting a family-centered strategy. Families are engaged in the eradication of mosquito breeding sites by monitoring, inspecting, and eliminating mosquito larvae. The program mandates that each household designate an individual to be responsible for larva monitoring, a concept referred to as “Satu Rumah Satu Jumantik” (“One House One Mosquito Larva Inspector”) [7]. Nevertheless, the support of health volunteers continues to be necessary for effective monitoring.
- Similar to their position in Thailand [8], health volunteers play a significant role in Indonesia due to their direct engagement with primary health care providers and neighboring communities. Health volunteers play a crucial role in dengue control efforts in. They coordinate with primary health care to be larva monitoring teams, which are responsible for inspecting homes and public areas for larvae. They also provide health education to families and communities, and they diligently record and report larval surveillance data on a weekly and monthly basis. These actions are comparable to those of a prior research conducted in Thailand, which included standard procedures including assessments of larvae, the elimination of mosquito breeding grounds, and efforts to reduce dengue deaths [9].
- Several factors could influence dengue prevention behavior, including knowledge, perceptions, the involvement of family members, the roles of health volunteers, and employment status [2,10-14]. People with strong understanding of dengue vector control measures were 7.62 times more likely than adults with low knowledge to display good overall preventative behavior regarding dengue vector breeding control measures [13]. Those with a positive perception are often more likely to engage in effective prevention behaviors [2].
- Recommendations from health volunteer influenced community participation in carrying out mosquito nest eradication behavior. As many as 70.7% of respondents participated in dengue prevention practiced because of recommendations from health volunteers [14]. Building dengue community capacity is crucial to creating a long-term strategy for eliminating dengue. According to the findings, the model with a high dengue community capacity level demonstrated little risk on the entomological and epidemiological dengue indexes [15]. Health volunteers are part of the dengue community capacity, under the “One House One Mosquito Larva Inspector” program, are expected to act as coordinators, overseeing and encouraging larval inspectors in each household. Consequently, health volunteers are anticipated to exhibit better prevention behaviors than the general population. Therefore, this study aimed to identify factors associated with the knowledge, attitudes, and practices (KAP) of dengue prevention behavior among health volunteers.
INTRODUCTION
- Study Setting
- This research was conducted in an urban area of Malang, Indonesia, from November 2017 to April 2018. Malang is divided into 5 sub-districts, which are further subdivided into 57 villages. For this study, 2 villages from each sub-district were randomly selected. From the total of 10 selected villages, 40 health volunteers were randomly recruited from each village for the study.
- Study Design
- This was a cross-sectional study with 400 respondents selected based on a previous study [2]. The study enrolled female health volunteers since all health volunteers in Indonesia are female. Respondents aged 18 and above who had resided in Malang for at least one year were included in this study. Trained enumerators administered the KAP questionnaire to the participants.
- Measures
- To explore KAP regarding dengue prevention, data were collected using a semi-structured questionnaire administered through face-to-face interviews. The questionnaire was adapted from a previous study [2] and was pre-tested for validity. Reliability was assessed using the Cronbach’s alpha coefficient, yielding scores of 0.59 for knowledge, 0.61 for practice, and 0.87 for attitude.
- Knowledge was assessed through open-ended questions. There were 4 questions in total, with the first and third questions each offering 3 points for correct answers, leading to a maximum score of 3 for these questions. If respondents provided only 1 or 2 correct responses, their knowledge was considered partially accurate. The maximum possible knowledge score was 8. Respondents scoring 7-8 were categorized as having more accurate knowledge (code 1), while those scoring between 0 and 6 were considered to have less accurate knowledge (code 0).
- Attitudes were assessed using a Likert scale-based tool, with a maximum score of 56. Attitudes were deemed more positive (coded as 1) if the score exceeded 47, and less positive (coded as 0) if the score ranged from 14 to 47. The highest possible score for prevention behavior was 35. Practices were categorized as more frequent best practices (coded as 1) if the score was above 25, and as less frequent best practices (coded as 0) if the score fell between 7 and 25. The cut-off for these variables was established based on the mean. Table 1 presents a comprehensive list of the questions and codes utilized in this study to evaluate KAP.
- We categorized participants into two age groups: young and middle adults (17-45 years, code 0), and senior adults (over 45 years, code 1). Formal education was divided into 2 levels: elementary school and junior secondary school (code 0), and high school or higher (code 1). Marital status was classified as married (code 0) and unmarried (code 1). For employment, participants were categorized as housewives (code 0) and workers (code 1). Monthly family income was categorized as less than 2.5 million Indonesian rupiah (IDR) (code 0) and more than 2.5 million IDR (code 1). We also divided the duration of being a health volunteer into two categories: 0-15 years (code 0) and over 15 years (code 1). Lastly, we inquired about the history of dengue in both the health volunteers and their families. The response options were “yes” or “no” (no=0, yes=1).
- Statistical Analysis
- Descriptive statistics were presented as frequencies and percentages. Data analysis was conducted using Stata version 14 (StataCorp., College Station, TX, USA). Multiple logistic regression was employed to quantify the associations between socio-demographic factors and KAP. All results were reported as odds ratios (ORs) with 95% confidence intervals (CIs).
- Ethics Statement
- This study was approved by the Ethics Committee of the Faculty of Medicine, Universitas Brawijaya Malang (No. 404/EC/KEPK/12/2017). Respondents in this study provided written informed consent for publication.
METHODS
KAP regarding dengue prevention
Socio-demographic factors
- Socio-demographic Factors
- Table 2 presents socio-demographic factors and KAP regarding dengue prevention. All 400 respondents were female, with 65.7% aged over 45 years. The majority were married (85.3%) and identified as housewives (81.0%). A significant portion had completed senior high school (64.0%) and had 0-15 years of experience as health volunteers (66.3%). Approximately 61.0% reported an average total family income 1-3 milion IDR per month. Approximately 79.3% had households comprising 1-5 people. Most respondents reported no previous history of dengue illness, either personally (95.7%) or among their family members (76.7%). Regarding KAP, 51.7% of the respondents demonstrated less accurate knowledge, 52.3% had less positive attitudes, and 62.8% engaged in dengue prevention practices infrequently.
- Knowledge, Attitudes, and Practices Regarding Dengue Prevention
- Table 3 presents the questions related to KAP concerning dengue prevention. The majority of respondents demonstrated good knowledge about the cause of dengue (79.5%). Although the level of knowledge regarding dengue prevention activities was 76.5%, only 13.3% of participants accurately described the “One House One Mosquito Larva Inspector” program.
- The majority of respondents exhibited a more positive attitude towards dengue prevention overall. Over 90% of participants (combining those who strongly agreed and agreed) held positive views regarding the severity of dengue, the benefits of prevention, cues to action, and the maintenance of dengue prevention measures. A significant portion of them strongly agreed (58.0%) and agreed (40.5%) that dengue is a dangerous disease that can lead to death. However, there was a less positive attitude towards perceived barriers related to cleaning and replacing water containers in bathrooms. Only 3.0% of respondents strongly agreed, and 5.7% agreed, that regularly cleaning water containers is time-consuming.
- Meanwhile, fewer than 40% (37.2%) of health volunteers engaged in best practices for dengue prevention more frequently. The best practice most commonly reported as always being performed by the majority of respondents was the reporting of their surveillance activities (75.8%), followed by cleaning water containers in the bathroom at least once a week (65.2%). Conversely, the practice of examining mosquito larvae in the surrounding neighborhood was only carried out by 52.2% of the volunteers. This finding indicates that improvement is needed in this area, as health volunteers have the responsibility to monitor their local environment.
- Multiple Logistic Regression Results
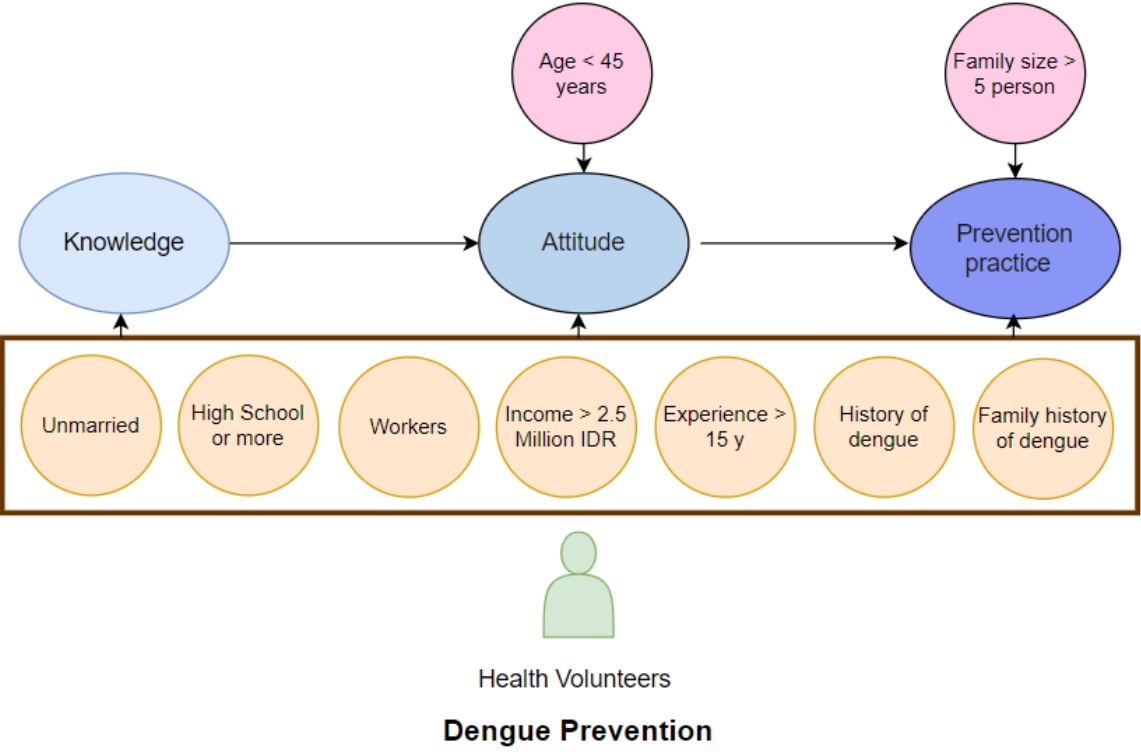
- Table 4 presents the results of a multiple logistic regression analysis examining the relationships of variables with KAP regarding dengue prevention. Two socio-demographic factors showed significant associations with attitudes. Specifically, possessing more accurate knowledge about dengue was associated with a 2.24-fold increase in the likelihood of having a positive attitude toward dengue prevention. Furthermore, forty percent reduction in positive attitude was observed in those over 45 years compared to those 17-45 years. In addition, the practice of dengue prevention was influenced by both the number of family members and the individual’s attitude. Households with more than 5 members had 1.90 times higher odds of adhering to dengue prevention best practices. Similarly, a more positive attitude was linked to a 1.69-fold increase in the likelihood of consistently engaging in recommended prevention practices.
RESULTS
- This study found no association between socio-demographic factors and knowledge. This contrasts with a study in Malaysia [16] that reported an association between ethnicity and occupation with knowledge. The discrepancy may be due to differing socio-demographic characteristics between the 2 studies. Our study did not differentiate participants by ethnicity, and the majority were housewives.
- More than half of the respondents (51.7%) demonstrated an average level of knowledge, which aligns with findings from other studies [2,11]. This could be attributed to the fact that the majority of respondents typically receive information about dengue from their primary healthcare providers, as was also observed in a previous study [2]. Health volunteers, who are tasked with promoting dengue awareness in their communities [8,9], may consequently possess more knowledge about the disease than the general population.
- A previous study revealed that 85.6% of respondents were aware that mosquitoes act as vectors [17]. Among these respondents in this study, 79.5% identified mosquitoes as a cause of dengue, although some were not familiar with the specific species of mosquito involved. Conversely, the lowest level of knowledge pertained to the “One House One Mosquito Larva Inspector” program. This may be because the program was only recently introduced, and primary healthcare providers may not have communicated this information effectively, resulting in a lack of awareness among health volunteers. Another study [18] also found that the community possessed a fair understanding of preventive measures, which aligns with the findings of this study.
- The multivariable analysis indicated that individuals under the age of 45 and those with a high level of knowledge were associated with a more positive attitude. Similar findings in Malaysia [16] and Nepal [19] have shown a positive correlation between knowledge and attitude although the degree of correlation was fair <0.5. The attitude of respondents, whether positive or negative, can be influenced by their level of knowledge. In turn, knowledge about dengue fever can impact attitudes toward dengue prevention. Additionally, younger individuals are more likely to have received a good education in recent times, which may influence their level of knowledge. A previous study discovered that participant education level was an independent predictor of attitude level [20].
- Approximately 47.7% of respondents held a more positive attitude towards dengue. The majority of health volunteers in this study exhibited a positive attitude regarding the severity of dengue, agreeing that it is a dangerous disease that can lead to death. Supporting this view, another studies revealed that individuals considered dengue to be a severe and potentially fatal disease [2,19,21]. Furthermore, the majority of health volunteers expressed a willingness to contribute to dengue control efforts, which is consistent with findings from another study [16].
- Attitudes were associated with practices in this study, aligning with previous studies in Indonesia [2,22]. According to prior research, individuals with positive perceptions were more likely to engage in effective dengue prevention behaviors [2,22,23]. However, unlike previous studies, this study did not find a direct association between knowledge and practice which similar with previous studies [2,20]. Most research participants already possessed a good level of knowledge, which might be attributed to the study being conducted during the rainy season—a time when dengue fever is more prevalent. Although health education initiatives can indeed raise public awareness about dengue during an outbreak, they are likely insufficient on their own to sustain larva monitoring efforts [22].
- It was found that the practice of dengue prevention was associated with the number of family members in a household. This result aligns with findings from other study [2]. A previous study indicated that respondents from households with more than 4 people, as well as those from households with 3-4 people, practiced prevention more effectively than those only 1-2 people in household [2]. This could be due to the additional help from family members in carrying out household chores and dengue prevention measures. Another factor could be that larger families have access to a wider range of sources for dengue knowledge and share this information among themselves [2]. Indeed, the presence of many family members appears to place a significant responsibility on parents or guardians, compelling them to maintain a clean and safe home environment.
- As members of the healthcare community, health volunteers are expected to demonstrate better practices than the general population. They are also tasked with organizing their neighborhoods to adopt the routine of eliminating mosquito breeding sites within their homes. However, according to this survey, only 37.2% of the volunteers engaged in effective dengue prevention practices. A previous study [24] found that just 25% of health volunteers adhered to excellent larva monitoring practices in their neighborhood, and 42.5% followed good practices for eradicating mosquito larvae. These suboptimal results may be attributed to the volunteers’ lack of information and their negative attitudes. Indeed, they often did not see it as their responsibility to encourage community involvement in larva monitoring as well previous study reported that community do not think they are at least partly responsible for dengue control [12].
- Additionally, 95.7% had never experienced dengue themselves. The lack of personal experience with dengue among health volunteers who practiced poor prevention behaviors might be explained by their own lack of illness from the disease. A prior study suggested that individuals are more likely to engage in good practices if they perceive a higher risk of becoming ill [11]. This implies that because they did not perceive themselves at risk, they practiced poor prevention behaviors. This study identified a specific behavior in need of improvement: the use of mosquito repellent or coils before going to bed in the morning or evening. The volunteers believed that there were not many mosquitoes in their vicinity, which led them to think that using repellents or mosquito coils was unnecessary.
- There are limitations to this study; firstly, the KAP levels were only evaluated once, which may not reflect changes over time. Additionally, these KAP levels were based on self-assessment, which could introduce bias into the actual responses. However, the study demonstrated that a positive attitude is an important factor affecting the practice of dengue prevention. Therefore, to alter people’s preventative practices, it is essential to change their perceptions of dengue. Healthcare practitioners must develop an appropriate and effective strategy to shift people’s perceptions of dengue infection. Sustainable promotion and training for the “One House One Mosquito Larva Inspector” initiative are essential, particularly among young health volunteers, to improve dengue prevention behaviors both within their own homes and in the surrounding environment.
DISCUSSION
-
Conflict of Interest
The authors have no conflicts of interest associated with the material presented in this paper.
-
Funding
This work was supported by the Faculty of Medicine of Universitas Brawijaya.
-
Author Contributions
Both authors contributed equally to conceiving the study, analyzing the data, and writing this paper.
Notes
Acknowledgements

- 1. Zuhriyah L, Habibie I, Baskoro A. The key container of Aedes aegypti in rural and urban Malang, East Java, Indonesia. Health Environ J 2012;3(3):51-58
- 2. Rakhmani AN, Limpanont Y, Kaewkungwal J, Okanurak K. Factors associated with dengue prevention behaviour in Lowokwaru, Malang, Indonesia: a cross-sectional study. BMC Public Health 2018;18(1):619. https://doi.org/10.1186/s12889-018-5553-zArticlePubMedPMC
- 3. Dinas Kesehatan Kota Malang. Health profile of Malang City in the year 2017 [cited 2024 Mar 10]. Available from: https://dinkes.malangkota.go.id/wp-content/uploads/sites/104/2018/11/Profil-Kesehatan-Kota-Malang-Tahun-2017.pdf (Indonesian)
- 4. Karyanti MR, Uiterwaal CS, Kusriastuti R, Hadinegoro SR, Rovers MM, Heesterbeek H, et al. The changing incidence of dengue haemorrhagic fever in Indonesia: a 45-year registry-based analysis. BMC Infect Dis 2014;14: 412. https://doi.org/10.1186/1471-2334-14-412ArticlePubMedPMC
- 5. Pratamawati DA. The role of Juru Pantau Jentik in dengue haemorrhagic fever early warning system in Indonesia. Natl Public Health J 2012;6(6):243-248. (Indonesian)
- 6. Kusriastuti R, Sutomo S. Evolution of dengue prevention and control. Dengue Bull 2005;29: 1-7
- 7. Rakhmani AN, Zuhriyah L, Nugraha RY. Community empowerment regarding “One House Onejumantik” program in Karang Besuki sub-district, Malang City. J Community Health Prev Med 2021;1(1):24-29. https://doi.org/10.21776/ub.jochapm.2021.001.01.4Article
- 8. Nontapet O, Maneerattanasak S, Jaroenpool J, Phumee A, Krachai W, Napet P, et al. Understanding dengue solution and larval indices surveillance system among village health volunteers in high- and low-risk dengue villages in southern Thailand. One Health 2022;15: 100440. https://doi.org/10.1016/j.onehlt.2022.100440ArticlePubMedPMC
- 9. Suwanbamrung C, Thoutong C, Eksirinimit T, Tongjan S, Thongkew K. The use of the “Lansaka Model” as the larval indices surveillance system for a sustainable solution to the dengue problem in southern Thailand. PLoS One 2018;13(8):e0201107. https://doi.org/10.1371/journal.pone.0201107ArticlePubMedPMC
- 10. Chandren JR, Wong LP, AbuBakar S. Practices of dengue fever prevention and the associated factors among the Orang Asli in Peninsular Malaysia. PLoS Negl Trop Dis 2015;9(8):e0003954. https://doi.org/10.1371/journal.pntd.0003954ArticlePubMedPMC
- 11. Wong LP, Shakir SM, Atefi N, AbuBakar S. Factors affecting dengue prevention practices: nationwide survey of the Malaysian public. PLoS One 2015;10(4):e0122890. https://doi.org/10.1371/journal.pone.0122890ArticlePubMedPMC
- 12. Mayxay M, Cui W, Thammavong S, Khensakhou K, Vongxay V, Inthasoum L, et al. Dengue in peri-urban Pak-Ngum district, Vientiane capital of Laos: a community survey on knowledge, attitudes and practices. BMC Public Health 2013;13: 434. https://doi.org/10.1186/1471-2458-13-434ArticlePubMedPMC
- 13. Sayavong C, Chompikul J, Wongsawass S, Rattanapan C. Knowledge, attitudes and preventive behaviors related to dengue vector breeding control measures among adults in communities of Vientiane, capital of the Lao PDR. J Infect Public Health 2015;8(5):466-473. https://doi.org/10.1016/j.jiph.2015.03.005ArticlePubMed
- 14. Puspareni NL, Patra IM, Rusminingsih NK. Impact determinant factors on community participation to eradicate dengue mosquito nest in Panjer District in the year 2012. J Environ Health 2014;4(1):70-74. (Indonesian)
- 15. Suwanbamrung C, Dumpan A, Thammapalo S, Sumrongtong R, Phedkeang P. A model of community capacity building for sustainable dengue problem solution in Southern Thailand. Health 2011;3(9):584-601. https://doi.org/10.4236/health.2011.39100Article
- 16. Selvarajoo S, Liew JW, Tan W, Lim XY, Refai WF, Zaki RA, et al. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: a cross-sectional study. Sci Rep 2020;10(1):9534. https://doi.org/10.1038%2Fs41598-020-66212-5ArticlePubMedPMC
- 17. Paz-Soldán VA, Morrison AC, Cordova Lopez JJ, Lenhart A, Scott TW, Elder JP, et al. Dengue knowledge and preventive practices in Iquitos, Peru. Am J Trop Med Hyg 2015;93(6):1330-1337. https://doi.org/10.4269/ajtmh.15-0096ArticlePubMedPMC
- 18. Alobuia WM, Missikpode C, Aung M, Jolly PE. Knowledge, attitude, and practices regarding vector-borne diseases in western Jamaica. Ann Glob Health 2015;81(5):654-663. https://doi.org/10.1016/j.aogh.2015.08.013ArticlePubMed
- 19. Dhimal M, Aryal KK, Dhimal ML, Gautam I, Singh SP, Bhusal CL, et al. Knowledge, attitude and practice regarding dengue fever among the healthy population of highland and lowland communities in central Nepal. PLoS One 2014;9(7):e102028. https://doi.org/10.1371/journal.pone.0102028ArticlePubMedPMC
- 20. Phuyal P, Kramer IM, Kuch U, Magdeburg A, Groneberg DA, Lamichhane Dhimal M, et al. The knowledge, attitude and practice of community people on dengue fever in Central Nepal: a cross-sectional study. BMC Infect Dis 2022;22(1):454. https://doi.org/10.1186/s12879-022-07404-4ArticlePubMedPMC
- 21. Shuaib F, Todd D, Campbell-Stennett D, Ehiri J, Jolly PE. Knowledge, attitudes and practices regarding dengue infection in Westmoreland, Jamaica. West Indian Med J 2010;59(2):139-146PubMed
- 22. Mohamad M, Selamat MI, Ismail Z. Factors associated with larval control practices in a dengue outbreak prone area. J Environ Public Health 2014;2014: 459173. https://doi.org/10.1155/2014/459173ArticlePubMedPMC
- 23. Harapan H, Rajamoorthy Y, Anwar S, Bustamam A, Radiansyah A, Angraini P, et al. Knowledge, attitude, and practice regarding dengue virus infection among inhabitants of Aceh, Indonesia: a cross-sectional study. BMC Infect Dis 2018;18(1):96. https://doi.org/10.1186/s12879-018-3006-zArticlePubMedPMC
- 24. Putri YD. Prevention of dengue by dengue larva monitoring (Jumantik) and relationship with larva-free number in Rawa Buntu primary health care south Tangerang City in 2016 [dissertation]. Kota Tangerang Selatan: Syarif Hidayatullah Jakarta Islamic State University. 2017 (Indonesian)
 PubReader
PubReader ePub Link
ePub Link Cite
Cite