
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 47(1); 2014 > Article
-
Original Article
Factors Predicting the Physical Activity Behavior of Female Adolescents: A Test of the Health Promotion Model - Hashem Mohamadian1, Mohammad Ghannaee Arani2
-
Journal of Preventive Medicine and Public Health 2014;47(1):64-71.
DOI: https://doi.org/10.3961/jpmph.2014.47.1.64
Published online: January 29, 2014
1Research Centre for Health-Related Social Determinates, Department of Public Health, School of Health, Kashan University of Medical Sciences, Kashan, Iran.
2Trauma Research Centre, Kashan University of Medical Sciences, Kashan, Iran.
- Corresponding author: Mohammad Ghannaee Arani, MSc. Ghotb-e-Ravandi Blvd, Kashan, Iran. Tel: +98-913-3622326, Fax: +98-361-5551112, mohammadarani@yahoo.com
• Received: August 8, 2013 • Accepted: December 31, 2013
Copyright © 2014 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
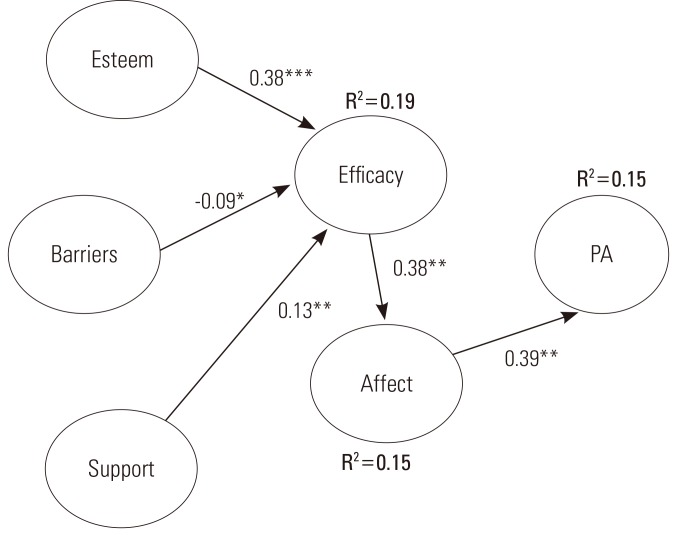
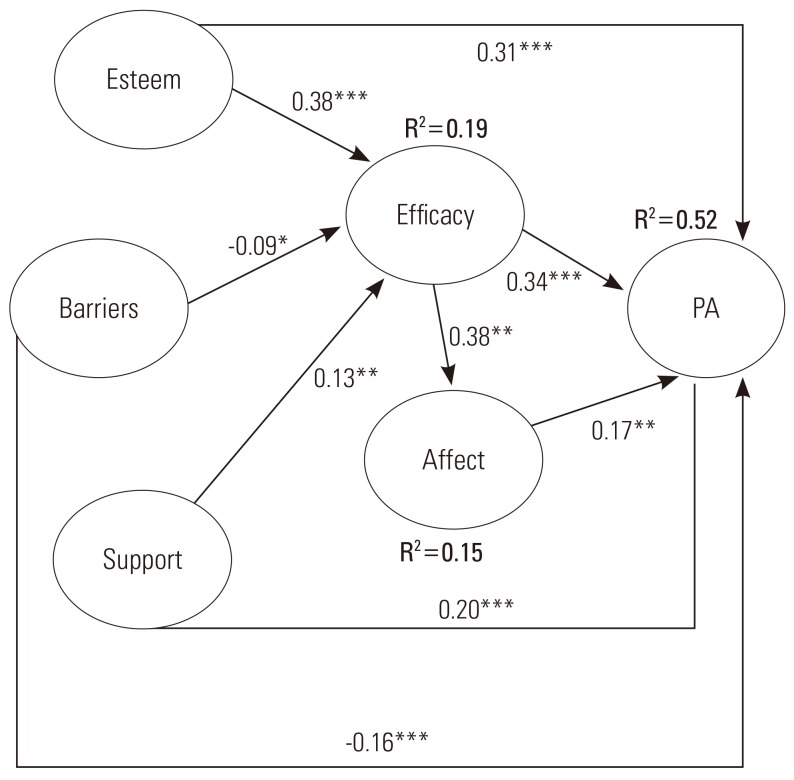
Figure & Data
References
Citations
Citations to this article as recorded by 
- A meta-analysis of the relationship between social support and physical activity in adolescents: the mediating role of self-efficacy
Hao Lin, Haidong Chen, Qingzao Liu, Jie Xu, Shan Li
Frontiers in Psychology.2024;[Epub] CrossRef - Modelo de Nola Pender para promoção da saúde do adolescente
Daniela Bulcão Santi, Iara Sescon Nogueira, Vanessa Denardi Antoniassi Baldissera
REME-Revista Mineira de Enfermagem.2023;[Epub] CrossRef - Evaluation of Physical Activity and its Effective Factors in Junior High School Female Students in Rafsanjan City: Application of Social-cognitive Theory, 2017-18
Zahra Soleiman Ahari, Mohammad Asadpour, Leili Mazar, Mostafa Nasirzadeh
Qom Univ Med Sci J.2021; 15(3): 188. CrossRef - Predicting physical activity among urban adolescent girls: A test of the health promotion model
Vicki R. Voskuil, Lorraine B. Robbins, Steven J. Pierce
Research in Nursing & Health.2019; 42(5): 392. CrossRef - Health behaviours in emerging adulthood: Their relationship with perceived maternal and paternal parental attitudes and the mediating role of self-efficacy
Anna Maria Jankowska, Marta Łockiewicz, Dorota Dykalska-Bieck, Ariadna Łada, Weronika Owoc, Dawid Stańczykowski
Health Psychology Report.2017; 6(1): 94. CrossRef - The relationship between self-esteem and overall health behaviors in Korean adolescents
Junghyun Park, Young-Ho Kim, Seon-Joo Park, Sooyeon Suh, Hae-Jeung Lee
Health Psychology and Behavioral Medicine.2016; 4(1): 175. CrossRef - Should Schools Send BMI Report Cards to Parents? A Review of Literature
Alexander Henningsen, Piroska Boros, Kent Ingvalson, Fabio E. Fontana, Oksana Matvienko
Journal of Physical Education, Recreation & Dance.2015; 86(9): 26. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


