
Articles
- Page Path
- HOME > J Prev Med Public Health > Volume 55(1); 2022 > Article
-
Original Article
Mediating Effect of Cognitive Function on the Relationship Between Geriatric Oral Health and Quality of Life Among Korean Seniors -
Eun Jee Chang1
 , Hyun-Jae Woo2, Kyu-Hyoung Jeong3
, Hyun-Jae Woo2, Kyu-Hyoung Jeong3 -
Journal of Preventive Medicine and Public Health 2022;55(1):106-113.
DOI: https://doi.org/10.3961/jpmph.21.536
Published online: January 12, 2022
1Department of Preventive Medicine, Graduate School of Public Health, Seoul National University, Seoul, Korea
2Seoul Metropolitan Council, Seoul, Korea
3Department of Social Welfare, Semyung University, Jecheon, Korea
- Corresponding author: Kyu-Hyoung Jeong, Department of Social Welfare, Semyung University, 65 Semyung-ro, Jecheon 27136, Korea E-mail: jqbrother@semyung.ac.kr
Copyright © 2022 The Korean Society for Preventive Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objectives
- Previous studies have found that the oral health of seniors can affect their physical nutrition and quality of life (QoL). Additionally, poor oral health can lead to the development of dementia, which is associated with decreased cognitive function. This study aimed to examine the impact of geriatric oral health (GOH) on the QoL of Korean seniors and the mediating effects of cognitive function.
-
Methods
- We used data from the seventh Korean Longitudinal Study of Aging conducted in 2018. In total, 4049 seniors were included in our study. We analyzed the impact of GOH on QoL according to 5 mediating domains of cognitive function and control variables. To examine each path of mediating effects, bootstrapping with 5000 iterations was performed with 95% confidence intervals.
-
Results
- Our findings revealed that good GOH had a positive effect on the QoL of seniors. Also, better GOH corresponded to a higher degree of cognitive function within all 5 domains: orientation, memory registration, attention/calculation, memory recall, and language and visuospatial ability. In addition, 3 domains of the 5 domains (attention/calculation, memory recall, and language and visuospatial ability) had significant mediating effects on the relationship between GOH and QoL.
-
Conclusions
- This study suggests that adequate management of GOH is crucial for promoting a better QoL and a high degree of cognitive function among seniors. To prevent cognitive impairment, such as dementia, future studies should take a more targeted approach by examining data according to each cognitive domain and various socio-demographic factors.
- The proportion of individuals aged 65 years and older in Korea reached 15.7% (approximately 8 125 000 people) in 2020. Oral health problems such as periodontal disease are some of the most commonly diagnosed conditions among seniors [1]. Geriatric oral health (GOH) is closely related to nutritional intake and interpersonal relationships, both of which affect the quality of life (QoL) [2,3]. In addition, several variables related to chewing ability, such as the occlusal force of the posterior teeth, tooth loss, and the use of dentures, also correlate with cognitive decline and the risk of dementia [4-6]. Cognitive decline causes depression and social isolation in seniors, which, like GOH, affect their QoL [7].
- Therefore, oral hygiene and cognitive health promotion programs are essential for improving seniors’ QoL [8]. Previous studies have used the Geriatric Oral Health Assessment Index (GOHAI) to identify the relationship between GOH and QoL [9,10]. However, findings on the effects of cognitive decline caused by GOH on QoL were inconclusive. Further, there are multiple domains of cognitive function, including orientation, memory, and concentration, for which diagnosis and treatment methods may vary depending on the level of deterioration within each domain. Nonetheless, no studies have analyzed each domain individually. Thus, this study aimed to comprehensively examine the effect of GOH on QoL and the mediating effect of cognitive function on their relationships to gather data supporting the development of an active GOH program.
INTRODUCTION
- Data
- Data from the seventh wave of the Korean Longitudinal Study of Aging (KLoSA) in 2018 were used to examine the effect of GOH on QoL and the mediating effect of cognitive function in seniors aged 65 years and older. The Korea Aging Research Panel Survey, a representative geriatric panel survey in Korea, was used to collect data on the demographic characteristics and health status of Korean seniors. This study included 4049 subjects aged 65 years and older from the seventh KLoSA for whom data were available on oral health, cognitive function, and QoL.
- We used the GOHAI to assess oral health, which was the independent variable in this study. The GOHAI is an instrument that includes a 12-item questionnaire and is answered using a 6-point scale (1, always; 2, very often; 3, often; 4, sometimes; 5, seldom and 6, never). A higher GOHAI score indicates a higher QoL related to oral health [11,12]. The Cronbach’s α value for all items related to oral health was 0.860.
- The dependent variable in this study was QoL, which was measured using the subjects’ answers to a 5-item life satisfaction questionnaire from the seventh KLoSA. Each item assessed the respondents’ health status, economic status, relationships with their spouses, relationships with their children, and overall QoL. Total possible scores ranged from 0 to 100 and were calculated in 10-point increments, and a higher score indicated a higher degree of life satisfaction. Life satisfaction is the most critical indicator of an individual’s subjective QoL. Thus, life satisfaction and subjective QoL have been used interchangeably in previous studies [13]. We used the average score for the 5-item life satisfaction questionnaire from the seventh KLoSA as a proxy for QoL to comprehensively evaluate the physical, mental, and socioeconomic effects of oral health and cognitive function on QoL. The Cronbach’s α value for all items was 0.844.
- In this study, scores for each of the 5 domains of cognitive function (orientation of time and place, memory registration, attention/calculation, memory recall, and language and visuospatial ability) were measured using the Korean Mini-Mental State Examination (K-MMSE) [14,15]. The K-MMSE [16] is a 30-point questionnaire that is widely used in clinical and research settings to measure cognitive decline and dementia [17]. The total possible scores for each domain are 10 points for orientation, 3 points for memory registration, 5 points for attention/calculation, 3 points for memory recall, and 9 points for visuospatial ability. A higher score indicates a higher degree of cognitive function.
- The control variables for this study were gender, age, education level, household income, and area of residence. For gender, 0 and 1 were assigned as dummy variables for men and women, respectively, and age was considered a continuous variable. For education level, dummy variables of 1, 2, 3, and 4 were assigned for “elementary school or lower,” “middle school,” “high school,” and “undergraduate or higher,” respectively. Household income was considered a continuous variable, but the responses were log-transformed to conform to normality. For residential districts, dummy variables of 0 and 1 were assigned to dong districts, which are the administrative units that contain urban neighborhoods in Korea, and eup-myeon districts, which are the administrative units that contain rural towns in Korea, respectively.
- Statistical Analysis
- We confirmed the effects of GOH on QoL primarily by examining the mediating effect of cognitive function. A mediation effect model can take the regression analysis approach or the counterfactual approach. The regression analysis approach includes a traditional statistical model proposed by Baron and Kenny [18] that mainly uses a path diagram to graphically represent the regression equation derived from the structural relationship between the variables. Baron and Kenny proposed a 3-step approach. Step 1 shows how the independent variable X affects the dependent variable Y (path: X→Y). Step 2 tests the path X→M to examine the relationship between the independent variable X and the mediator M. Step 3 involves conducting multiple regression analysis to demonstrate how X and M affect Y simultaneously (path: X→Y, M→Y).
- The counterfactual model, proposed by Pearl [19] and VanderWeele and Vansteelandt [20], includes an integrated framework for causal inference and can analyze linear as well as non-linear and non-parametric structural equation models. This model is divided into the controlled direct effect, natural direct effect (NDE), natural indirect effect (NIE), and the total effect of NDE+NIE. Using the counterfactual model, an analysis of the interaction effects between the variables and the unmeasured confounding factors that are difficult to consider in the traditional model can be conducted.
- In this study, we used regression analysis approach due to its advantages related to exploratory model trimming and theory building. SPSS version 25.0 (IBM Corp., Armonk, NY, USA) was used for data processing and descriptive statistics. In addition, SPSS PROCESS Macro model 4, developed by Hayes [21], was used to confirm the effects of GOH and cognitive function on QoL and verify the multiple mediation effects of cognitive function subcategories. The PROCESS macro website (http://www.processmacro.org/) provides a free, downloadable file containing this model. Bootstrapping with 5000 iterations was conducted with 95% confidence intervals (CIs) to analyze each mediating effect.
- Ethics Statement
- In this study, we used KLoSA which is an open access source of secondary data. This data is available to anyone after logging in on the Korea Enployment Information Service website (https://survey.keis.or.kr/klosa/klosadownload/List.jsp). The data guarantees anonymity by using personal unique numbers to prevent exposure of personal information through personal identification. Therefore, it is possible to exempt from institutional review board approval and additional written consent since the risk of personal information leakage is very low.
METHODS
Independent variables
Dependent variables
Mediating variables
Control variables
- Demographic and Socioeconomic Characteristics
- A total of 4049 subjects were included in the present study, and their demographic characteristics are shown in Table 1. There were 1693 (41.8%) men and 2356 (58.2%) women, and the average age was 75.55 years (standard deviation [SD], 7.10). More than half of the subjects (n=2207, 54.5%), were elementary school graduates or under, and the annual average household income was approximately 22.1 million Korean won (SD, 22.8). A total of 2864 people (70.7%) resided in a dong district, whereas 1185 people (29.3%) resided in a eup-myeon district, with those who resided in a dong district exceeding the percentage of those who resided in a eup-myeon district by more than double. The average GOHAI score was 4.05 (SD, 0.72) out of 6, and the average QoL score was 58.89 (SD, 14.73) out of 100. The average scores for the domains of cognitive function were as follows: 8.94 (SD, 1.83) for orientation, 2.36 (SD, 0.91) for memory registration, 3.28 (SD, 1.84) for attention/calculation, 1.69 (SD, 1.07) for memory recall, and 7.35 (SD, 2.03) for language and visuospatial ability.
- Model Testing
- We used a total of 6 models to verify the effect of GOH on QoL and the mediating effects of the cognitive domains. In models 1 to 5, the effect of GOH on the cognitive domains was examined. In model 6, the effect of GOH and cognitive function on QoL was tested.
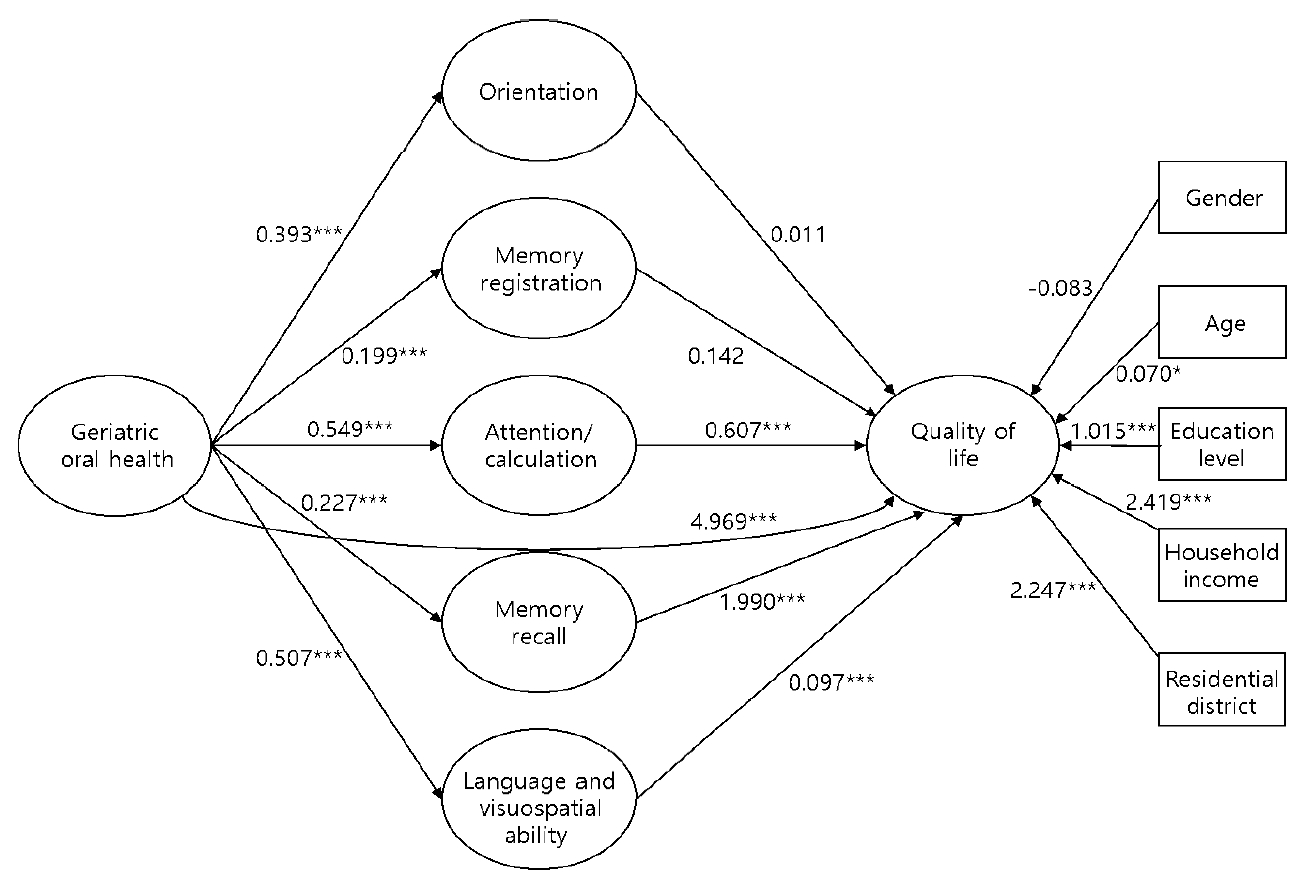
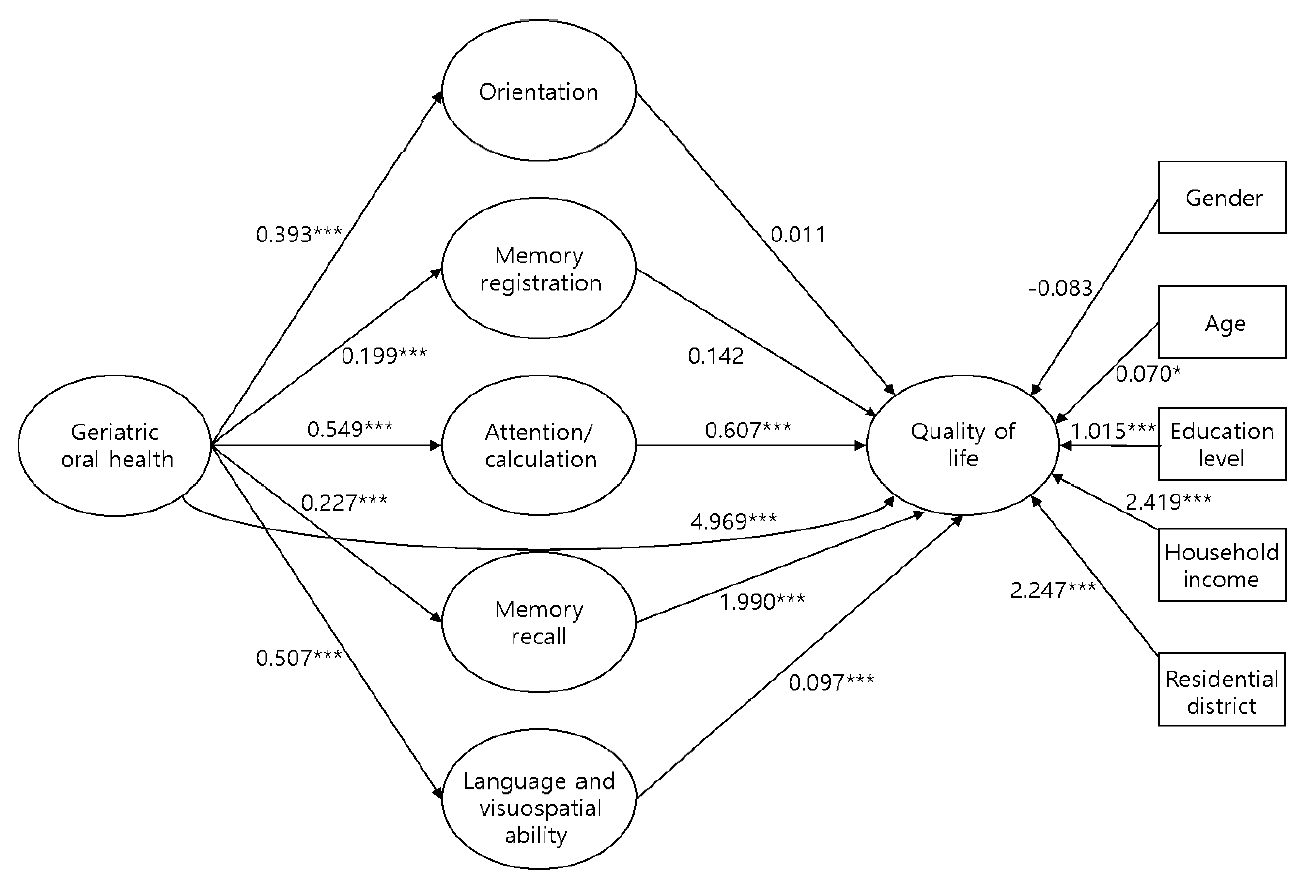
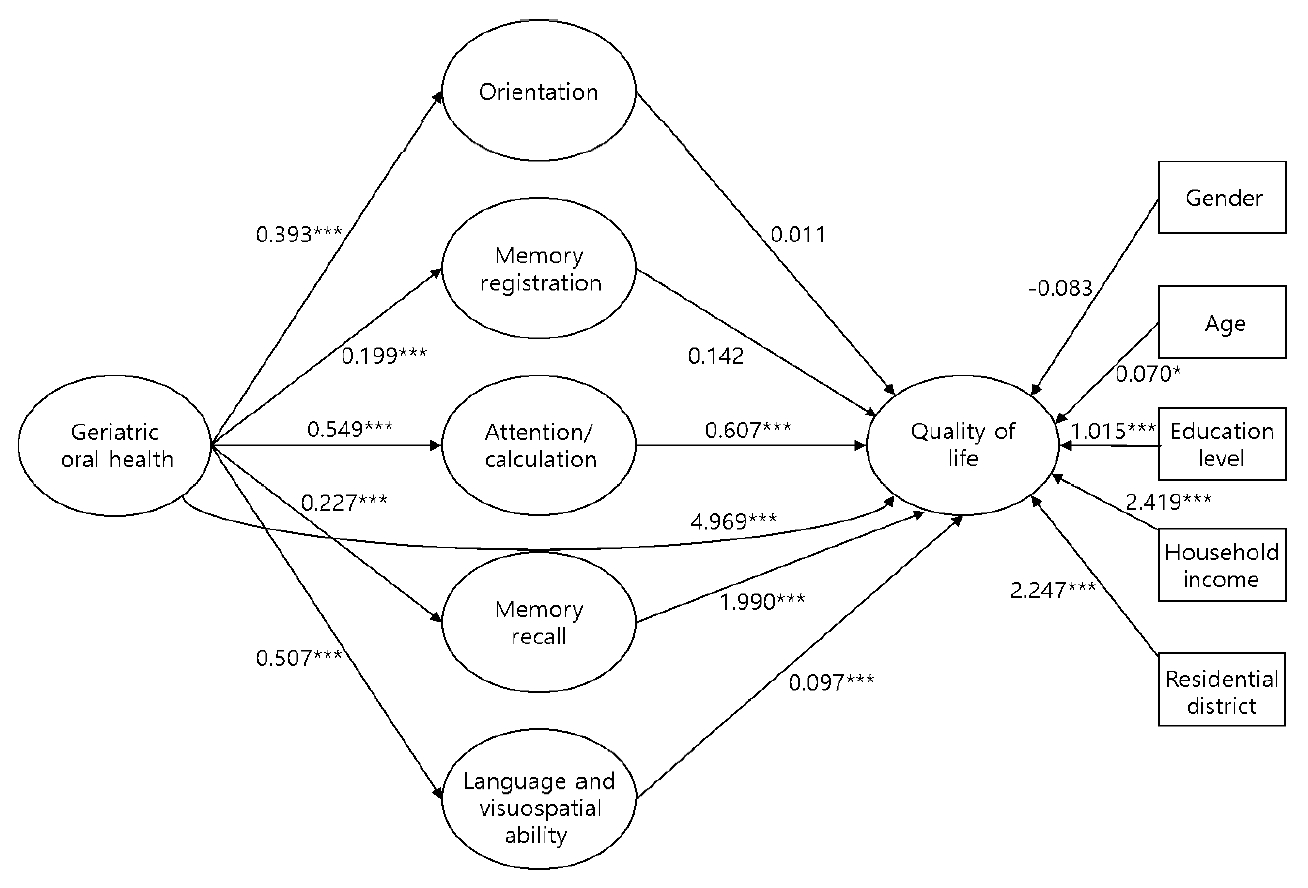
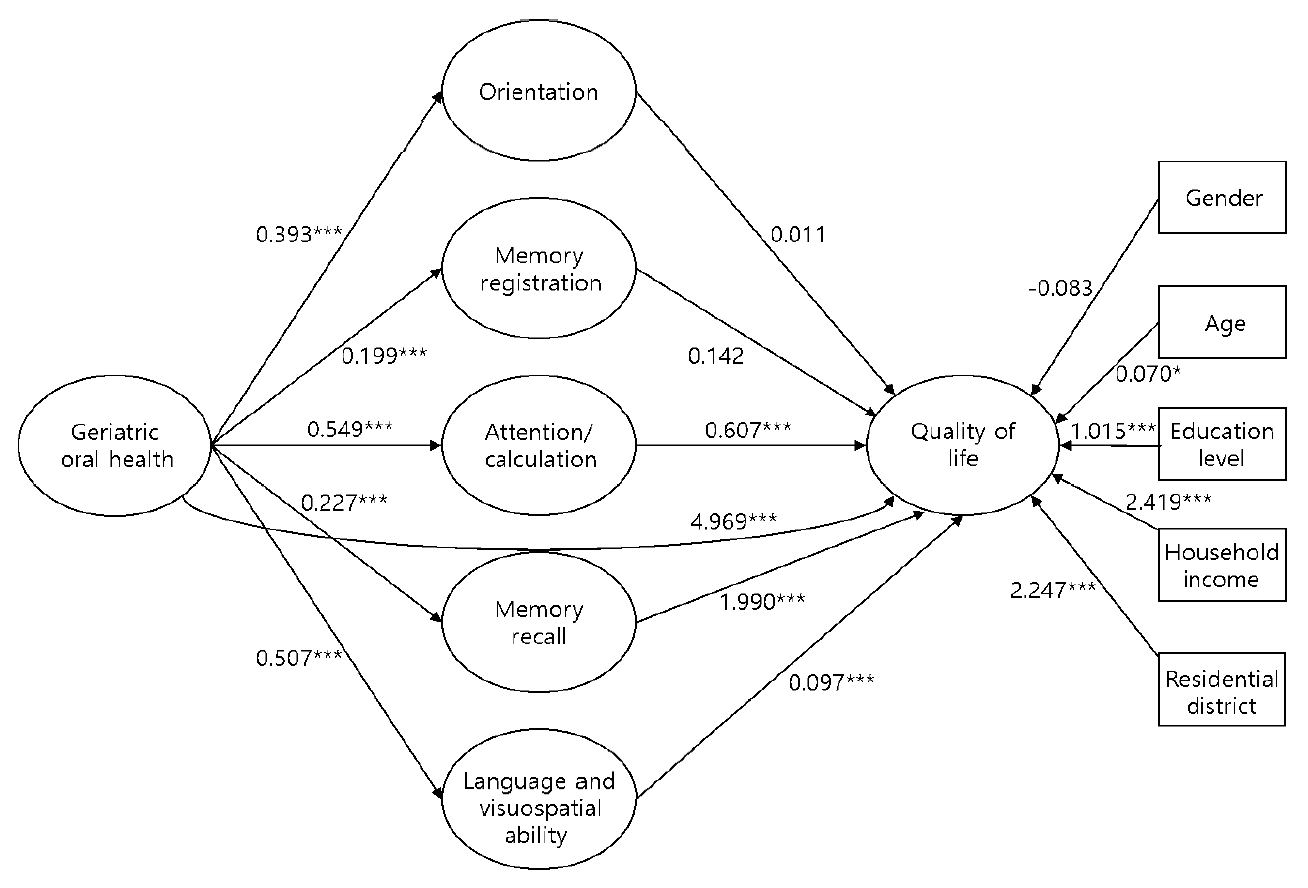
- Table 2 shows the results of the analysis of the effects of GOH on each cognitive function domain. The results were statistically significantly high for all parameters: orientation (coefficient=0.393, p<0.001), memory registration (coefficient=0.199, p<0.001), attention and calculation (coefficient=0.549, p<0.001), memory recall (coefficient=0.227, p<0.001), and language and visuospatial ability (coefficient=0.507, p<0.001). In other words, better oral health corresponded to a higher score for all 5 domains of cognitive function. Goodness-of-fit testing was undertaken for models 1 to 5 (p<0.001), and the effect size for each model was 17.4%, 16.4%, 25.1%, 18.1%, and 25.0%, respectively. Based on these results, the related effect sizes (R2) for model 3 (attention and calculation) and model 5 (language and visuospatial) were the highest, at approximately 25% (model 3: R2=0.251; model 5: R2=0.250). Scores for the 5 subcategories were significantly lower for the control variables, especially among females, older seniors, and subjects with a low education level. Orientation scores were significantly lower among subjects with a higher household income. In addition, scores for memory registration and language and visuospatial ability were lower among subjects who lived in dong administrative units than among those who lived in eup-myeon administrative units.
- Table 3 shows the results for model 6, in which the effect of GOH and the cognitive function subcategories on QoL were examined. The effect size for the dependent variable (QoL) was 26.9% (R2=0.269), and the model fit the data well (F=134.823, p<0.001). The analysis indicated that better GOH (coefficient=4.969, p<0.001) corresponded to a higher QoL, and the 3 cognitive function subcategories of attention/calculation (coefficient=0.607, p<0.001), memory recall (coefficient=1.990, p<0.001), and language and visuospatial ability (coefficient=0.907, p<0.001) had statistically significant effects on QoL. QoL tended to be lower among women, older seniors, subjects with a low educational level, subjects with a low household income, and subjects who lived in eup-myeon districts. These results were statistically significant for variables except for gender (Figure 1).
- Table 4 shows each of the 5 cognitive function subcategories arranged as parameters to verify the mediating effect of cognitive function on the relationship between GOH and QoL. The results suggest that the paths (oral health→attention/calculation→QoL), (oral health→memory recall→QoL), (oral health→language and visuospatial ability→QoL) were statistically significant since their 95% CIs didn’t contain values of 0. Meanwhile, the paths (oral health→orientation→QoL) and (oral health→memory registration→QoL) were not statistically significant since their 95% CIs contained values of 0.
RESULTS
- This study aimed to examine the effect of GOH on QOL and the mediating effect of cognitive function. Our findings show that GOH affects every subcategory of cognitive function. These results correspond to the results of previous studies in which poor oral health was found to lead to reduced chewing ability, which in turn affected cognitive function and brain activity related to memory and learning due to reduced blood flow in the brain [4-6]. Our results also reveal that GOH influences QOL. Previous studies have demonstrated that poor oral health can cause problems when consuming food and compromise systemic health, leading to health issues such as malnutrition, diabetes, and cardiovascular disorders. Poor oral health also can change the pronunciation and appearance of seniors which negatively affects interpersonal relationships [22,23]. In addition, three subcategories (attention/calculation, memory recall, language and visuospatial ability) were found to affect QOL along with GOH. Memory recall is a crucial area for determining cognitive decline, and a diagnosis of cognitive decline varies depending on the impairment of single or multiple domains [24]. Given that concentration, memory, and vocabulary are the main subcategories that adversely affect instrumental activities of daily living and participation in social activities, the diminished function of these areas may lower self-efficacy and self-esteem, causing social isolation, depression, and lower QOL [25]. Therefore, the statistically significant results for three subcategories of cognitive function support the findings of previous studies. The control variables (gender, age, education level, household income, residential districts) showed varying degrees of statistical significance related to cognitive function. Findings in the past also demonstrated that the degree of cognitive function differed according to the demographic characteristics, suggesting the need for education/training programs tailored with specific demographic profiles [25]. Lastly, gender, age, marital status, education level, and household income were found to statistically significantly affect geriatric QOL, which confirmed previous results [7].
- We suggest the following policy recommendations based on our study finidngs. First, the promotion of oral examinations, including routine scaling, is essential for preventing primary disorders that affect the QOL of seniors, such as periodontal disease and dry mouth. Second, the National Dementia Care Center and local dental clinics should collaborate to expand support related to the national oral health project and medical coverage for older patients with mild cognitive impairment and a high risk of dementia [26]. Third, it is vital to implement targeted pharmaceutical and non-pharmaceutical interventions according to the demographic characteristics of the individual and the patterns of cognitive decline for each domain of a cognitive function. Treatments, including music, exercise, behavioral therapy, occupational therapy, recall exercises, communication, and cognitive stimulation therapy, can be used in reference to the domain of cognitive function being addressed [27]. While women appeared to have a higher degree of cognitive decline and impaired QOL than men, their orientation, memory registration, memory recall, and language and visuospatial ability were found to improve significantly after social interaction [28]. Thus, health and welfare services combine diverse efforts to address the needs of all seniors according to their physical, mental, and socioeconomic conditions are necessary.
- There are several limitations in this study. First, due to the nature of utilizing cross-sectional data, a causal relationship cannot be inferred. Future studies should use longitudinal data to assess the relationships between GOH, QOL, and cognitive function. Second, the study subjects were likely limited to cognitively independent seniors since proxy surveys were not administered when the KLoSA was conducted. Future research should include subjects with severe cognitive impairment and classify them according to their risk of dementia. Third, due to small sample size, large-scale cohort data needs to be utilized to generalize the findings to elderly population of South Korea. Fourth, since the K-MMSE is a screening tool rather than a diagnostic tool, various cognitive function measurement tools should be used in the future to determine the effect size of the domains of cognitive function. Despite these limitations, our study identified the mediating effect of all domains of cognitive function on GOH and QOL, underlying the importance of adequate management of GOH for promoting a btter QOL among the elderly population [29-32].
DISCUSSION
SUPPLEMENTAL MATERIALS
-
CONFLICT OF INTEREST
The authors have no conflicts of interest associated with the material presented in this paper.
-
FUNDING
None.
Notes
ACKNOWLEDGEMENTS
-
AUTHOR CONTRIBUTIONS
Conceptualization: Chang EJ, Jeong KH. Data curation: Chang EJ, Woo HJ. Formal analysis: Chang EJ, Woo HJ. Funding acquisition: None. Methodology: Jeong KH. Project administration: Woo HJ. Visualization: Chang EJ. Writing – original draft: Chang EJ. Writing – review & editing: Woo HJ, Jeong KH.
Notes
| Variables |
Model 1 |
Model 2 |
Model 3 |
Model 4 |
Model 5 |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Oral health→Orientation |
Oral health→Memory registration |
Oral health→Attention/calculation |
Oral health→Memory recall |
Oral health→Language and visuospatial ability |
|||||||
| Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | ||
| Independent variable | |||||||||||
| Oral health | 0.393*** | 0.038 | 0.199*** | 0.019 | 0.549*** | 0.037 | 0.227*** | 0.022 | 0.507*** | 0.041 | |
| Control variables (ref: men) | |||||||||||
| Gender | -0.289*** | 0.058 | -0.068* | 0.029 | -0.402*** | 0.056 | -0.111*** | 0.034 | -0.346*** | 0.061 | |
| Age | -0.083*** | 0.004 | -0.034*** | 0.002 | -0.064*** | 0.004 | -0.039*** | 0.002 | -0.093*** | 0.004 | |
| Education level (ref.: elementary) | 0.084** | 0.031 | 0.086*** | 0.015 | 0.322*** | 0.029 | 0.142*** | 0.018 | 0.263*** | 0.033 | |
| Household income (logged) (10 000 KRW/y) | -0.097*** | 0.032 | -0.007 | 0.016 | 0.044 | 0.031 | 0.019 | 0.019 | -0.032 | 0.034 | |
| Residential districts (ref: dong) | -0.060 | 0.059 | -0.118*** | 0.030 | -0.005 | 0.057 | -0.049 | 0.034 | -.293*** | 0.062 | |
| Constant | 14.339 | 0.477 | 4.111 | 0.239 | 5.222 | 0.459 | 3.415 | 0.277 | 12.346 | 0.506 | |
| R2 | 0.174 | 0.164 | 0.251 | 0.181 | 0.250 | ||||||
| F-value | 141.634*** | 132.069*** | 226.069*** | 148.988*** | 224.342*** | ||||||
| Variables |
Model 6 |
||
|---|---|---|---|
|
Oral health and cognitive function→QoL |
|||
| Coefficient | SE | ||
| Independent variable | |||
| Oral health | 4.969*** | 0.300 | |
| Control variables | |||
| Gender (ref. men) | -0.083 | 0.442 | |
| Age | 0.070* | 0.033 | |
| Education level (ref. elementary) | 1.015*** | 0.237 | |
| Household income (logged) (10 000 KRW/y) | 2.419*** | 0.244 | |
| Residential districts (ref. dong) | 2.247*** | 0.449 | |
| Mediator | |||
| Orientation | 0.011 | 0.157 | |
| Memory registration | 0.142 | 0.311 | |
| Attention/calculation | 0.607*** | 0.148 | |
| Memory recall | 1.990*** | 0.260 | |
| Language and visuospatial ability | 0.907*** | 0.166 | |
| Constant | 0.858 | 4.035 | |
| R2 | 0.269 | ||
| F-value | 134.823*** | ||
| Path | B | SE |
95% CI |
|
|---|---|---|---|---|
| LL | UL | |||
| Oral health→Orientation→QoL | 0.004 | 0.069 | -0.131 | 0.139 |
| Oral health→Memory registration→QoL | 0.028 | 0.065 | -0.094 | 0.158 |
| Oral health→Attention/calculation→QoL | 0.334* | 0.087 | 0.165 | 0.503 |
| Oral health→Memory recall→QoL | 0.452* | 0.074 | 0.317 | 0.603 |
| Oral health→Language and visuospatial ability→QOL | 0.460* | 0.098 | 0.270 | 0.660 |
- 1. Korea Health Promotion Institute. 2021 Integrated community health promotion project (oral health) [cited 2021 May 14]. Available from: https://www.khealth.or.kr/kps/publish/list?menuId=MENU00890&page_no=B2017003 (Korean)
- 2. Cho MJ, Kim JY, Jung YS, Shin HE, Youn HY, Park TJ, et al. Can the number of functional teeth potentially affect cognitive function? J Korean Acad Oral Health 2018;42(2):52-58Article
- 3. Hur IG, Lee TY, Dong JK, Hong SH. The effects of dental prostheses to the quality of life among the elderly. J Korean Acad Prosthodont 2010;48(2):101-110. (Korean)Article
- 4. Shin HE, Cho MJ, Choi YH, Song KB. Evaluation of relationship between cognitive function and occlusal status in elderly individuals using the T-scan III® system. J Korean Acad Oral Health 2017;41(2):96-101. (Korean)Article
- 5. Shin HE, Chang IJ, Cho MJ, Song KB, Choi YH. Association between masticatory ability, oral health-related quality of life and cognitive function in the elderly population using structural equation modeling. J Korean Acad Oral Health 2018;42(4):159-166. (Korean)Article
- 6. Stein PS, Kryscio RJ, Desrosiers M, Donegan SJ, Gibbs MB. Tooth loss, apolipoprotein E, and decline in delayed word recall. J Dent Res 2010;89(5):473-477ArticlePubMedPMC
- 7. Hwang RI, Lim JY, Lee YW. A comparison of the factors influencing the life satisfaction of the elderly according to their cognitive impairment level. J Korean Acad Nurs 2009;39(5):622-631. (Korean)ArticlePubMed
- 8. Park S. A study on the demands of oral health and medical care policies for the elderly: focused on a perception investigation on the oral health industry [dissertation]. Seoul: Chung-Ang University; 2015. (Korean)
- 9. Park CS, Han YS. A study on oral health assessment index (GOHAI) and life satisfaction of the state of oral health project of the elderly in Jeonbuk Korea. J Korean Soc Dent Hyg 2017;17(4):555-564. (Korean)
- 10. Cho MJ, Jung EK, Shin HE, Shin AR, Jo HY, Choi YH, et al. Relationship between the number of functional teeth and Geriatric Oral Health Assessment Index (GOHAI) in elderly. J Korean Soc Den Hyg 2016;16(3):455-461. (Korean)Article
- 11. Atchison KA, Dolan TA. Development of the Geriatric Oral Health Assessment Index. J Dent Educ 1990;54(11):680-687ArticlePubMed
- 12. Shin SJ, Jung SH. A Korean version of the Geriatric Oral Health Assessment Index (GOHAI) in elderly populations: validity and reliability. J Korean Acad Oral Health 2011;35(2):187-195. (Korean)
- 13. Ferrans CE, Powers MJ. Psychometric assessment of the Quality of Life Index. Res Nurs Health 1992;15(1):29-38ArticlePubMed
- 14. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12(3):189-198PubMed
- 15. Kang Y, Na DL, Hahn S. A validity study on the Korean MiniMental State Examination (K-MMSE) in dementia patients. J Korean Neurol Assoc 1997;15(2):300-308. (Korean)
- 16. Yang S, Jeong K, Choi JS. Effects of social activities on cognitive function by gender difference among older adults: a nineyear longitudinal analysis in South Korea. Korean J Gerontol Soc Welf 2017;72(3):225-250. (Korean)
- 17. Pangman VC, Sloan J, Guse L. An examination of psychometric properties of the mini-mental state examination and the standardized mini-mental state examination: implications for clinical practice. Appl Nurs Res 2000;13(4):209-213ArticlePubMed
- 18. Jung S, Yang TS, Park J. Testing mediated moderation using moderated multiple regression: conceptual and methodological considerations. Korean J Psychol Gen 2019;38(3):323-346. (Korean)Article
- 19. Pearl J. Interpretation and identification of causal mediation. Psychol Methods 2014;19(4):459-481ArticlePubMed
- 20. VanderWeele TJ, Vansteelandt S. Mediation analysis with multiple mediators. Epidemiol Methods 2014;2(1):95-115ArticlePubMedPMC
- 21. Hayes AF. PROCESS: a versatile computational tool for observed variable mediation, moderation, and conditional process modeling. 2012 [cited 2021 May 14]. Available from http://www.afhayes.com/public/process2012.pdf
- 22. Hong SH. Factors influencing the elderly’s oral health related quality of life. J Korean Data Anal Soc 2016;18(1):475-496. (Korean)
- 23. Back JU, Lee YS. The relationship of oral state and dietary habit to health condition among elderly people. J Korean Acad Health Welf Elder 2010;1(3):75-89. (Korean)
- 24. Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund LO, et al. Mild cognitive impairment--beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med 2004;256(3):240-246ArticlePubMed
- 25. Kim JH. Moderating effects of relationships with adult-children and friends & neighbors on the relationship between cognitive function and the quality of life among older adults. J Fam Relat 2019;24(1):3-22. (Korean)Article
- 26. Yang JM, Song SE, Heo MH, Kim JH. Association between GOHAI (Geriatric Natural Health Assessment Index) and QoL (quality of life). Health Soc Welf Rev 2020;40(4):245-263. (Korean)
- 27. Cho E, Jung Y, Kim E. The study of relation between cognition function and motor skill in elderly women. Korean J Adapt Phys Activ 2016;24(4):89-99. (Korean)Article
- 28. Yang HK. Social activities and cognitive functioning of the Korean older adults. Korean Health Econ Rev 2020;26(4):73-104. (Korean)
- 29. Kim YO, Shim MS. Cognitive functions, instrumental activities of daily living, depression and quality of life in the elderly with mild cognitive impairment. J Korean Public Health Nurs 2015;29(2):219-230. (Korean)Article
- 30. Son YS. Correlation between denture use and cognitive function according to the mastication of the elderly. Swallowing Rehabil 2018;1(2):1-9. (Korean)Article
- 31. Kim YR, Heo SE, Jang K, Kang HK. Effects of general and oral health status on dementia in the elderly in some areas. J Korean Soc Dent Hyg 2021;21(2):151-158. (Korean)Article
- 32. Lee YM, Park NH. The effects of dementia prevention program on cognition, depression, self-esteem and quality of life in the elderly with mild cognitive disorder. Korean J Adult Nurs 2007;19(5):104-114. (Korean)
REFERENCES
Figure & Data
References
Citations
- Association of Denture Use and Chewing Ability with Cognitive Function Analysed Using Panel Data from Korea Longitudinal Study of Aging (2006–2018)
Nu-Ri Jun, Jae-Hyun Kim, Jong-Hwa Jang
Healthcare.2023; 11(18): 2505. CrossRef - Relationship Between Oral Health and Cognitive Impairment in the Older Adults of Bushehr City
Sedegheh Khedish, Akram Farhadi, Hassan Malekizadeh, Zahra Sadat Jalaliyan, Marzeah Mahmoodi, Behrang Poorkhan
South Medical Journal.2023; 26(1): 38. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Effect Modification of Kidney Function on the Non-linear Association Between Serum Calcium Levels and Cardiovascular Mortality in Korean Adults
- The Effect of Cognitive Impairment on the Association Between Social Network Properties and Mortality Among Older Korean Adults
- The Moderating Effect of Gender on the Relationship Between Self-neglect and Suicidal Ideation in Older Adults of Korea

